Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251026_002
From Right Ventricular Outflow Tract to Left Anterior Descending Artery: A Rare Coronary Complication Following Ventricular Premature Contraction Ablation
By Chi-Te Chou, Chi-Yao Huang, Ming-Jen Kuo, Yu-Cheng Hsieh
Presenter
Chi-Te Chou
Authors
Chi-Te Chou1, Chi-Yao Huang1, Ming-Jen Kuo1, Yu-Cheng Hsieh1
Affiliation
Taichung Veterans General Hospital , Taiwan1
View Study Report
CASE20251026_002
Coronary - Complication Management
From Right Ventricular Outflow Tract to Left Anterior Descending Artery: A Rare Coronary Complication Following Ventricular Premature Contraction Ablation
Chi-Te Chou1, Chi-Yao Huang1, Ming-Jen Kuo1, Yu-Cheng Hsieh1
Taichung Veterans General Hospital , Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
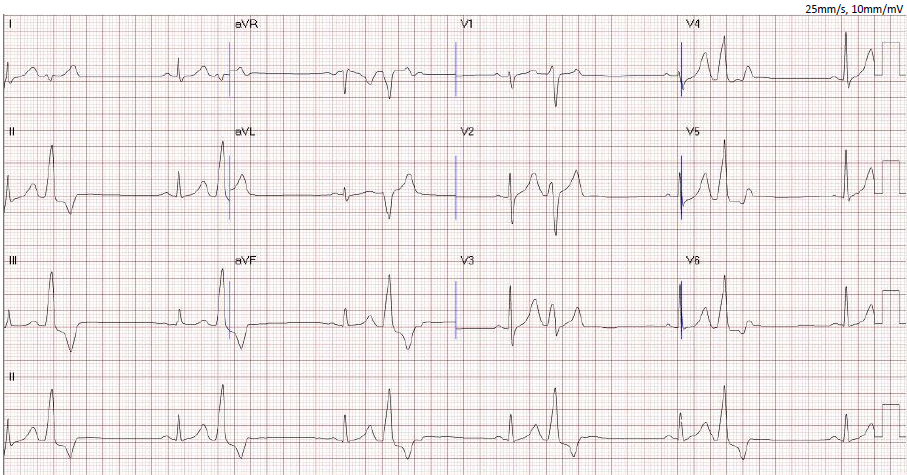
A 45-year-old man with no cardiac history presented with palpitations and frequent premature ventricular contractions (PVCs) on routine examination. Physical examination revealed irregular rhythm. Electrocardiography (ECG) demonstrated frequent PVCs with morphology suspected to originate from the right ventricular outflow tract (RVOT). Laboratory tests were unremarkable. 24-hour Holter monitoring showed a 40% PVC burden. Multidetector computed tomography (MDCT) revealed no coronary plaque.
Relevant Test Results Prior to Catheterization
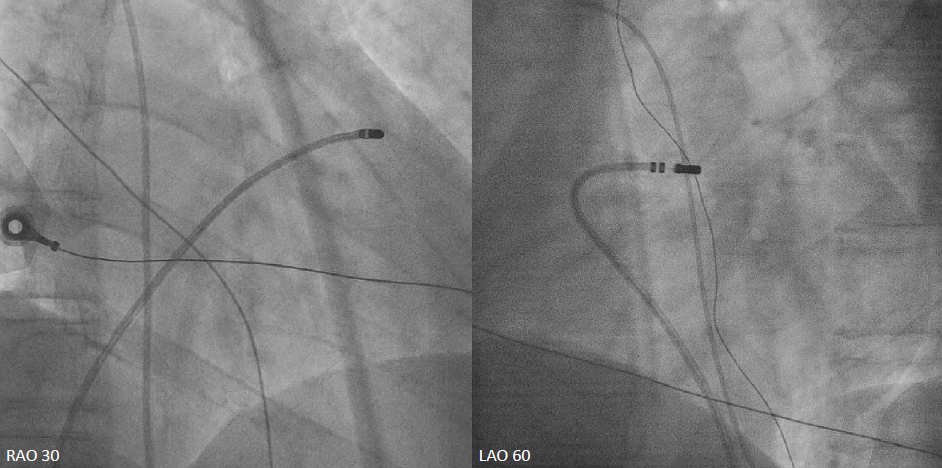
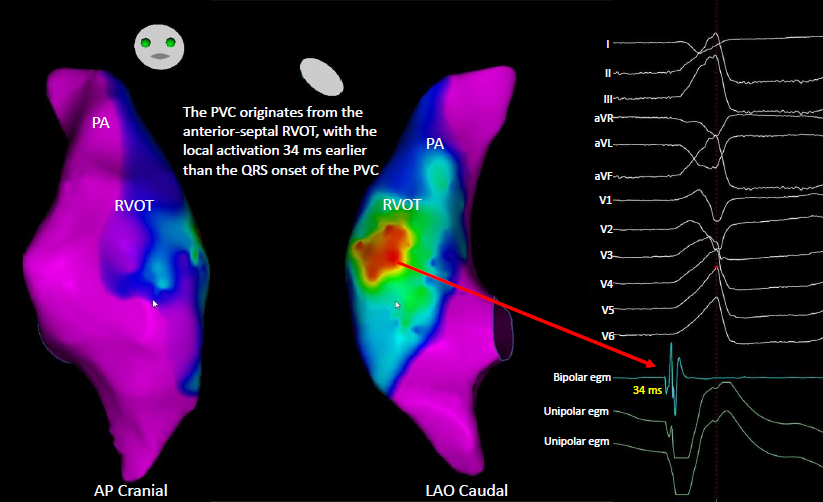
Three-dimensional electroanatomical mapping identified the PVC origin at the RVOT. Radiofrequency energy was delivered at multiple sites along the anteroseptal RVOT, resulting in complete elimination of PVC.Shortly after returning to the general ward post-ablation, the patient developed chest tightness and dyspnea. ECG showed ST-segment elevation in leads V1–V4, consistent with anterior wall ST-elevation myocardial infarction.

Relevant Catheterization Findings
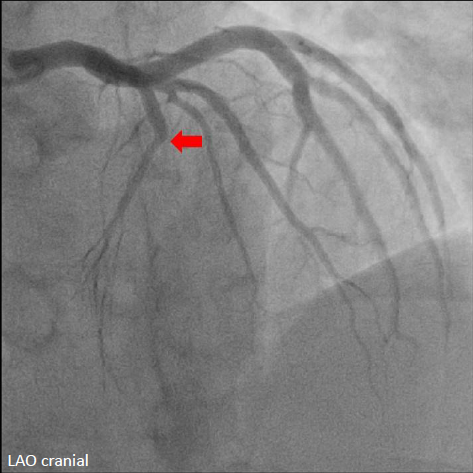
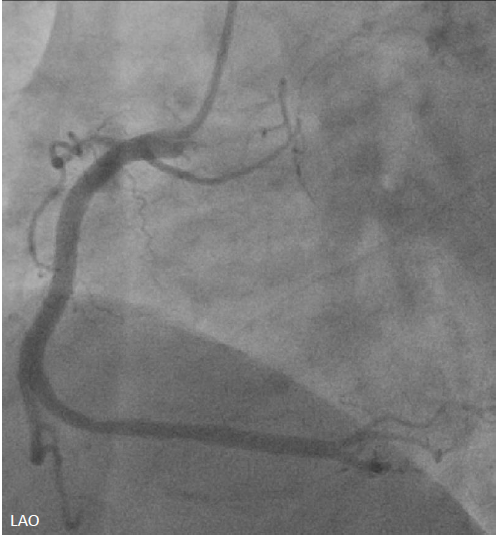
Emergent cardiac catheterization revealed patent left main coronary artery with total occlusion of the proximal left anterior descending artery (LAD). The left circumflex and right coronary arteries were patent. The culprit lesion was the proximal LAD.
 Diagnostic CAG.avi
Diagnostic CAG.avi
Diagnostic CAG RCA.avi
Interventional Management
Procedural Step
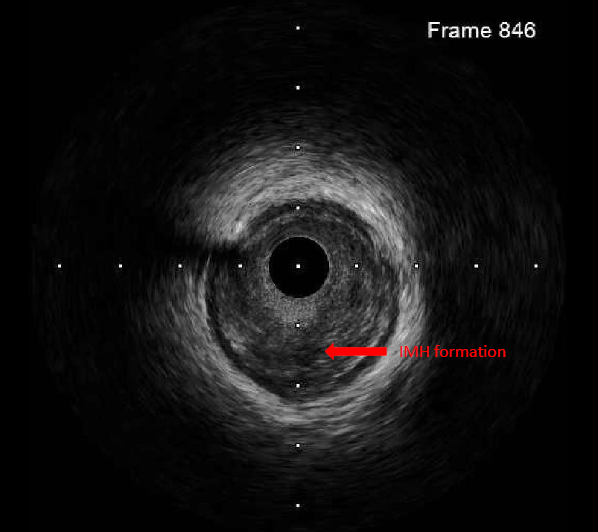
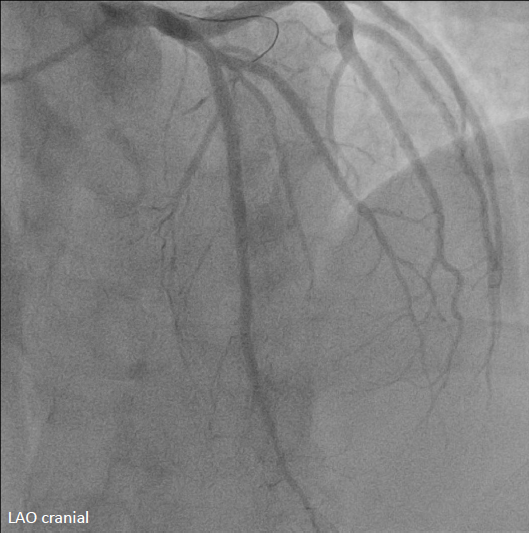
The left coronary artery was engaged with an XB 3.5×6 Fr guide catheter. Using a Fielder FC guidewire with a Fine-Cross microcatheter, the distal LAD was successfully accessed. Pre-dilation with a 1.5×20 mm balloon demonstrated residual stenosis with poor flow. Further dilation with a 2.0×15 mm balloon improved flow. Intravascular ultrasound (IVUS) revealed intramural hematoma (IMH) in the proximal-to-mid LAD. A drug-eluting stent (BMX6 2.75×33 mm) was deployed from the proximal LAD (distal to the first diagonal branch) to the mid LAD, followed by proximal post-stent dilation with a 4.0×12 mm non-compliant balloon at 4-16 atmospheres. Post-deployment IVUS confirmed adequate stent expansion without malapposition. Final coronary angiography demonstrated TIMI grade 3 flow.
Stent deployment.avi
Post stented IVUS.avi
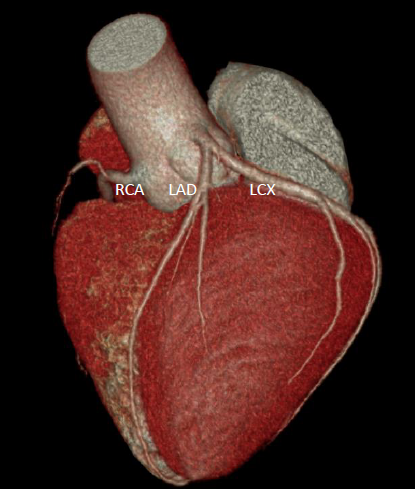
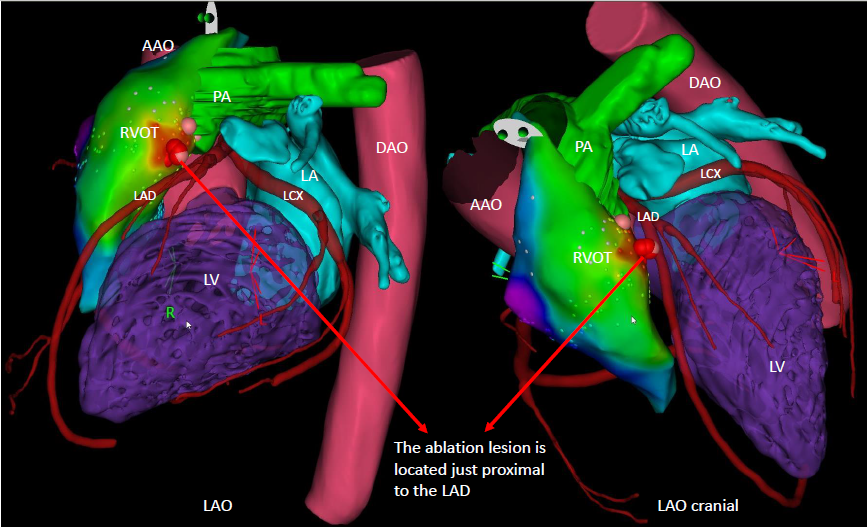
By integrating the MDCT coronary anatomy with the three-dimensional electroanatomical map and ablation lesion sites, it was demonstrated that the radiofrequency applications were directly adjacent to the proximal LAD, resulting in thermal injury and IMH formation.
Case Summary
This case underscores that LAD total occlusion can occur as a rare but serious complication of radiofrequency ablation at the anteroseptal RVOT, where the ablation site lies in close proximity to the proximal LAD. The underlying mechanism in this case was not atherosclerotic plaque rupture, but rather thermal injury leading to IMH formation. Importantly, prompt coronary intervention successfully restored coronary flow and preserved myocardial function.