Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251026_001
Anatomical Feasibility for a Tall-in-Tall Redo TAVI Strategy Using an Evolut Valve Within the Failed CoreValve
By Weiting Wang, Yin-Hwa Chen
Presenter
Weiting Wang
Authors
Weiting Wang1, Yin-Hwa Chen1
Affiliation
Taipei Veterans General Hospital, Taiwan1
View Study Report
CASE20251026_001
Structural - Aortic Valve Intervention - Valve in Valve TAVR
Anatomical Feasibility for a Tall-in-Tall Redo TAVI Strategy Using an Evolut Valve Within the Failed CoreValve
Weiting Wang1, Yin-Hwa Chen1
Taipei Veterans General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
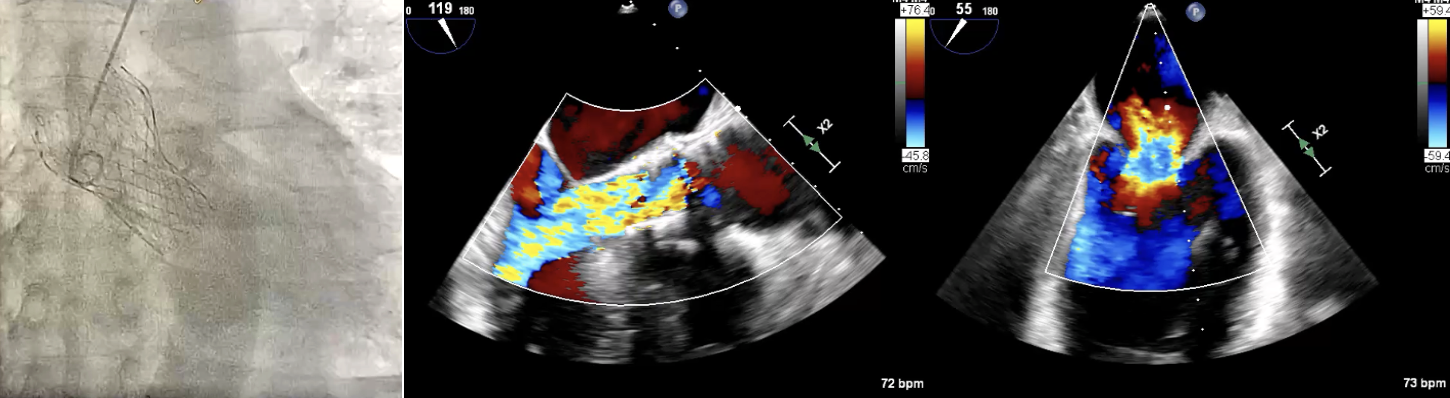
A 79-year-old male, who underwent TAVI with a 29 mm CoreValve in 2015, presented six years later with NYHA class III symptoms. Echocardiography showed Severe central AR and severe functional MR with Mean gradient: 12.4 mmHg; peak gradient: 23.3 mmHg, AVA: 1.4cm2 and LVEF: 61%. EuroSCORE II was 7.00% and STS score was 3.060%
Relevant Test Results Prior to Catheterization
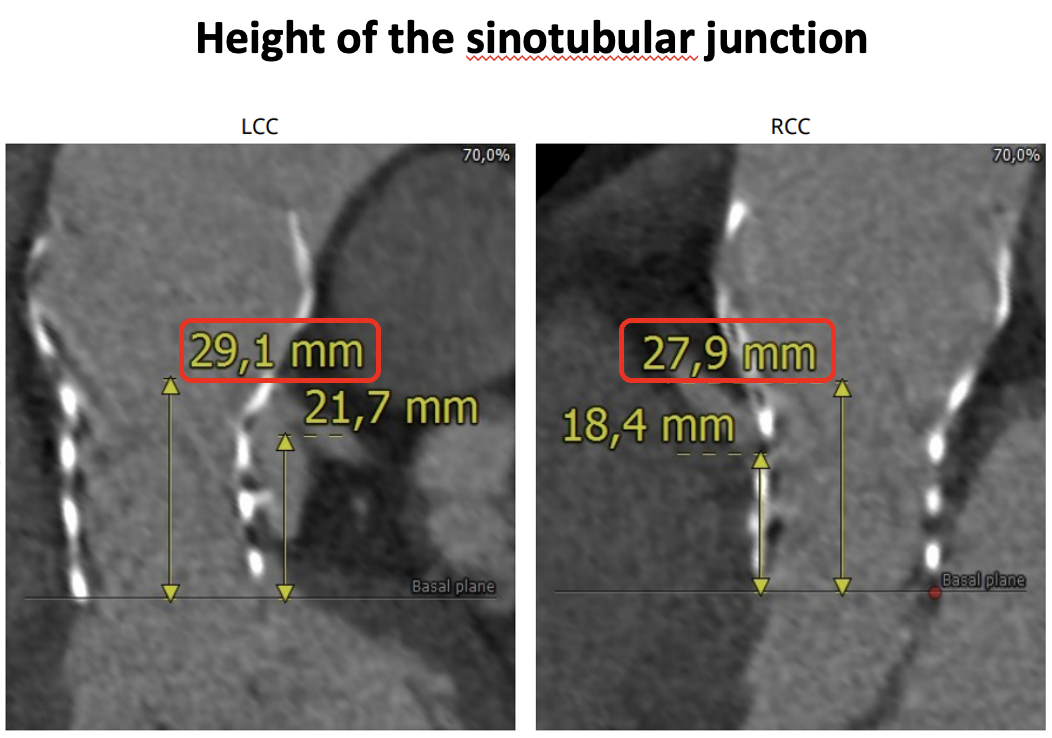
Multidetector CT was performed to assess the risk of coronary obstruction in the context of redo TAVI. The assessment focused on the spatial relationship between the neoskirt plane of the degenerated CoreValve and the coronary risk plane. The perimeter-derived annular diameter of failed CoreValve was 21.3 mm, guiding the selection of a 26-mm Evolut PRO valve. The narrowest valve-to-coronary distances measured 4.3 mm for the left main and 2.4 mm for the RCA.

Relevant Catheterization Findings
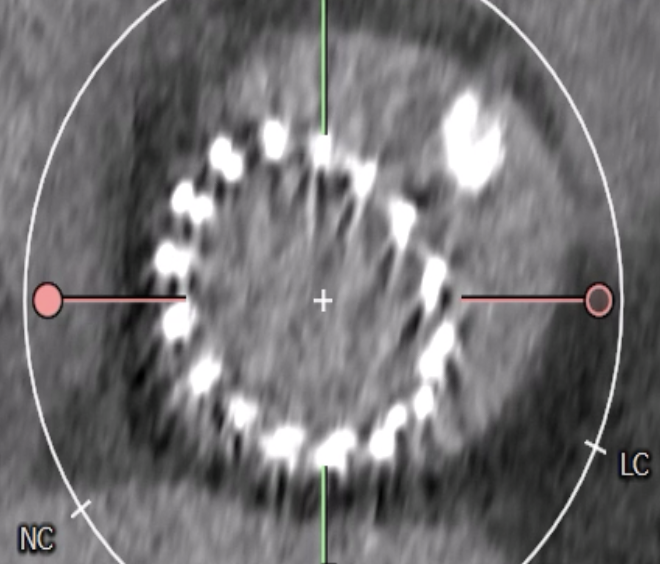
CT confirmed absence of commissural misalignment of failed CoreValve, and commissural alignment of the Evolut PRO was achieved by orienting the delivery system with the flush port at 3 o’clock. The inflow portion of the the Evolut PRO was implanted at the same level as the failed CoreValve. Aortography post-implantation confirmed no RCA obstruction.
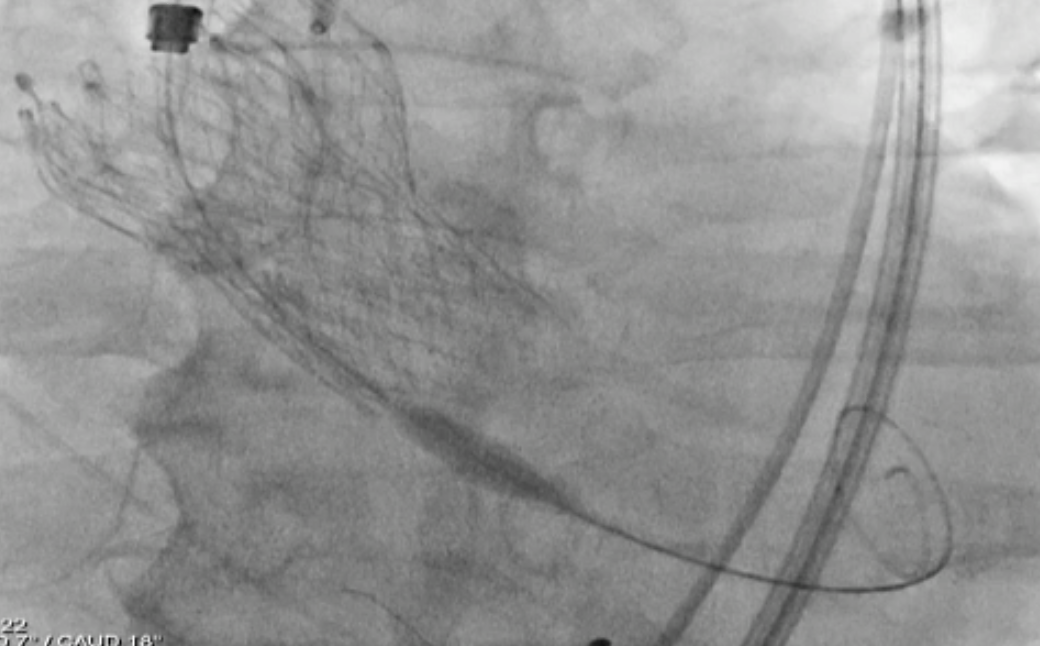
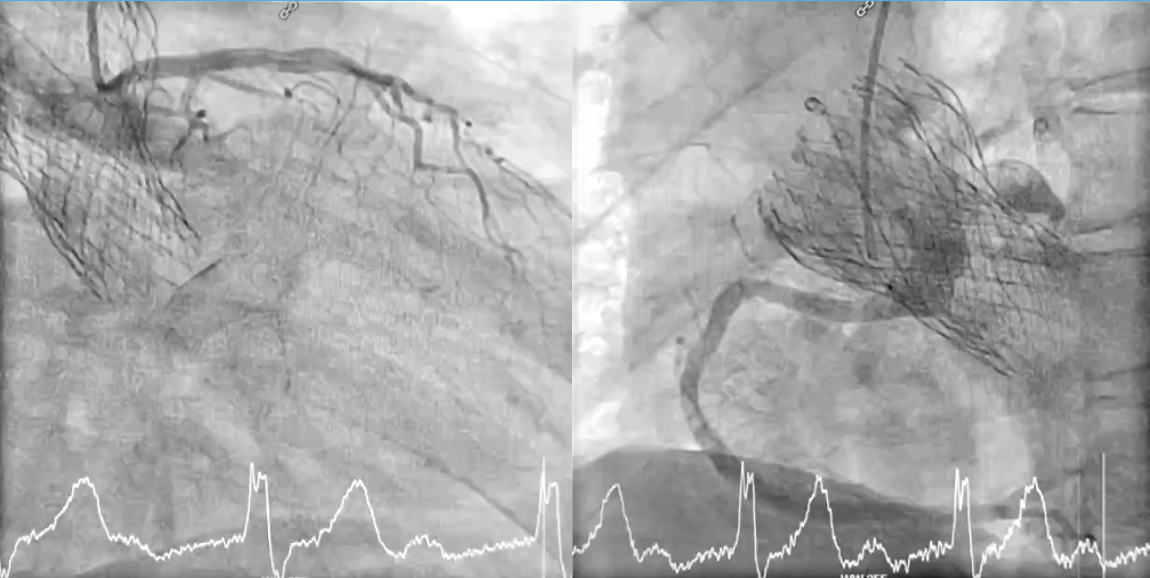
 post RedoTAVI CAG.png
post RedoTAVI CAG.png
TAVR_trim.mp4
Interventional Management
Procedural Step
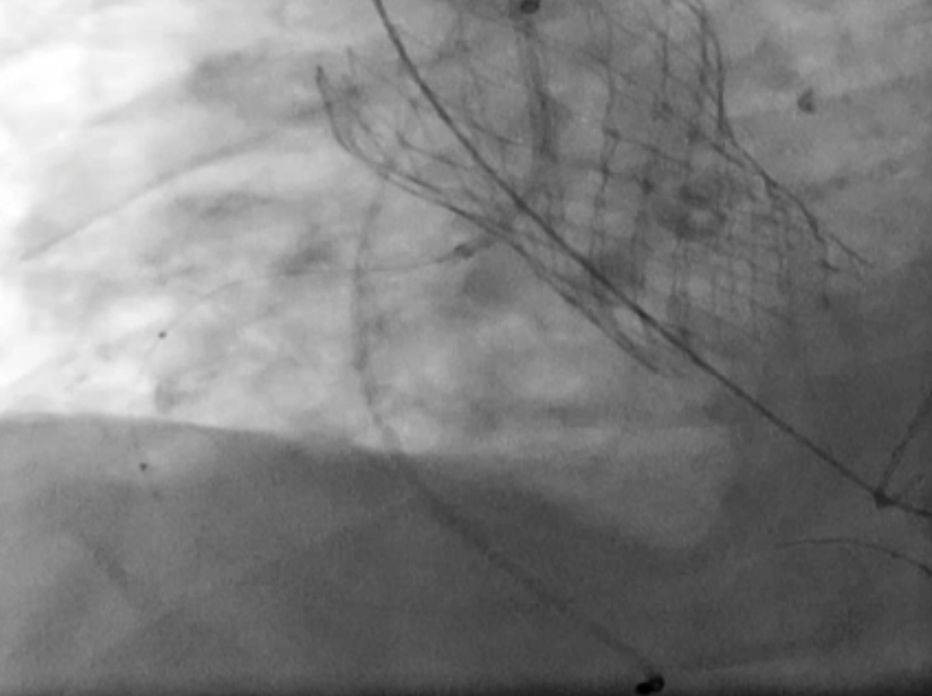
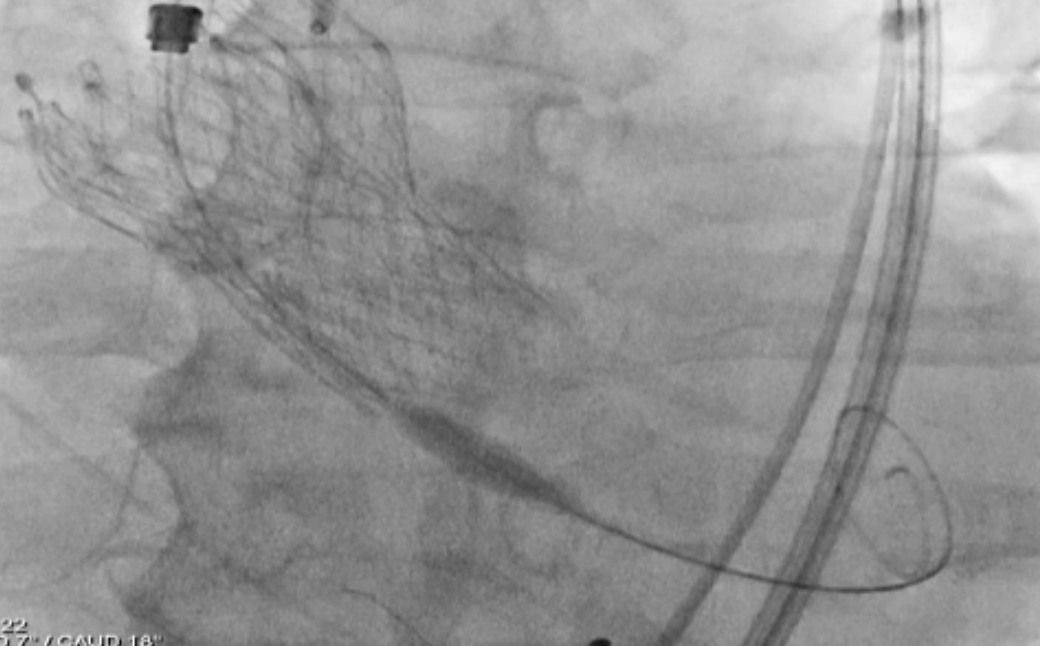
To mitigate the risk of coronary obstruction, the RCA was protected using a coronary guidewire and balloon. CT confirmed absence of commissural misalignment of failed CoreValve, and commissural alignment of the Evolut PRO was achieved by orienting the delivery system with the flush port at 3 o’clock. The inflow portion of the the Evolut PRO was implanted at the same level as the failed CoreValve. Aortography post-implantation confirmed no RCA obstruction, allowing safe removal of the guidewire and balloon. The procedure was uneventful, with no conduction disturbances or paravalvular leak. The functional mitral regurgitation resolved immediately after the procedure.
Case Summary
The tall-in-tall redo-TAVI approach is both feasible and effective, offering favorable hemodynamic outcomes and potential long-term durability. Its success depends on meticulous anatomical evaluation, particularly ensuring commissural alignment and maintaining a THV–STJ distance >2.0 mm to preserve future coronary access.