Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251024_002
Successful Repeat Percutaneous Intervention in Previously Stented Radial and Saphenous Vein Grafts: Technical Challenges to Achieve Favorable Outcomes
By Saurabh Goel, Ashish Goel
Presenter
Saurabh Goel
Authors
Saurabh Goel1, Ashish Goel2
Affiliation
Wockhardt Hospital, Mumbai Central, India1, Fayth Clinic, Mumbai, India2
View Study Report
CASE20251024_002
Coronary - Complex PCI - In-Stent Restenosis
Successful Repeat Percutaneous Intervention in Previously Stented Radial and Saphenous Vein Grafts: Technical Challenges to Achieve Favorable Outcomes
Saurabh Goel1, Ashish Goel2
Wockhardt Hospital, Mumbai Central, India1, Fayth Clinic, Mumbai, India2
Clinical Information
Relevant Clinical History and Physical Exam
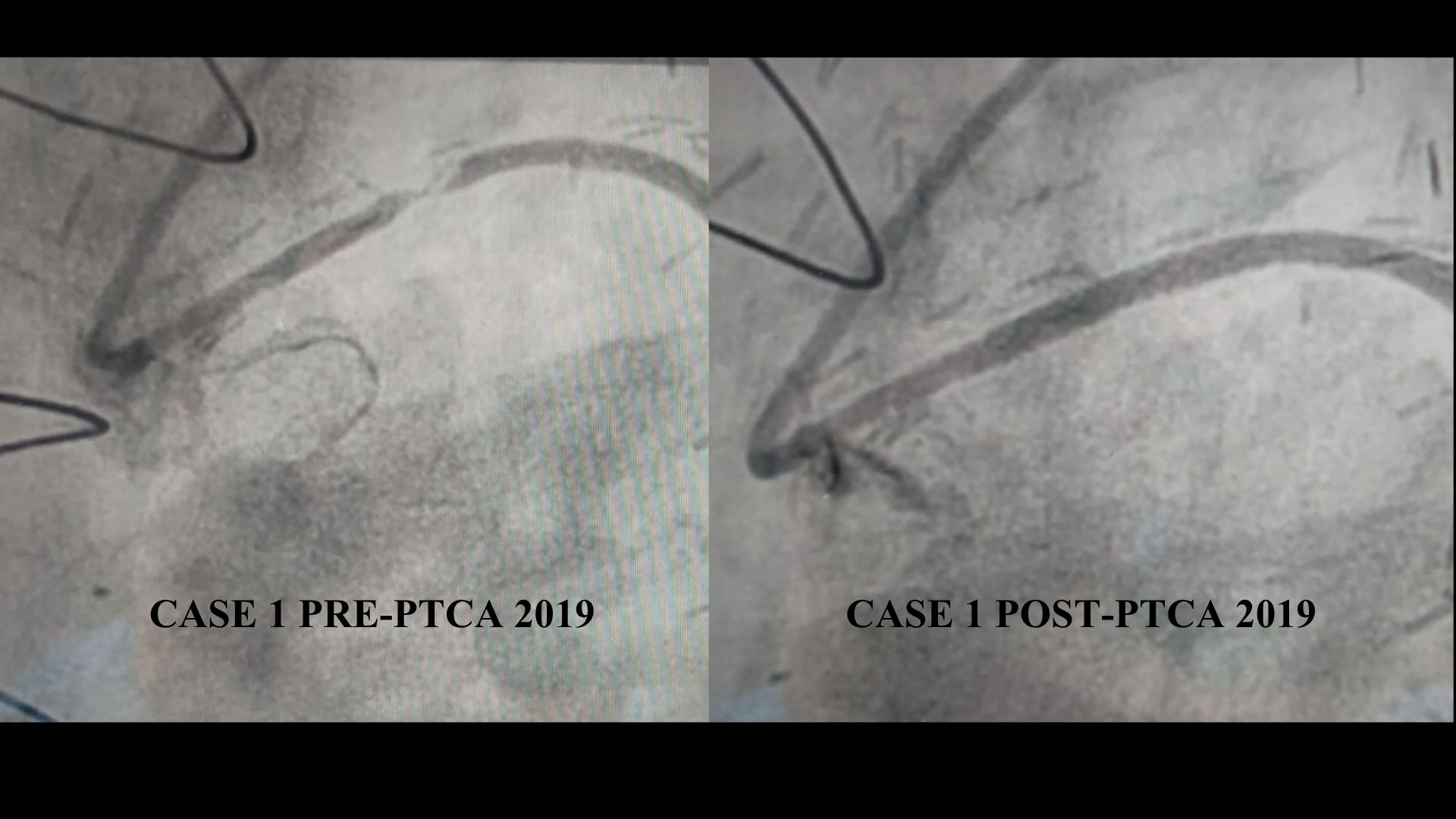
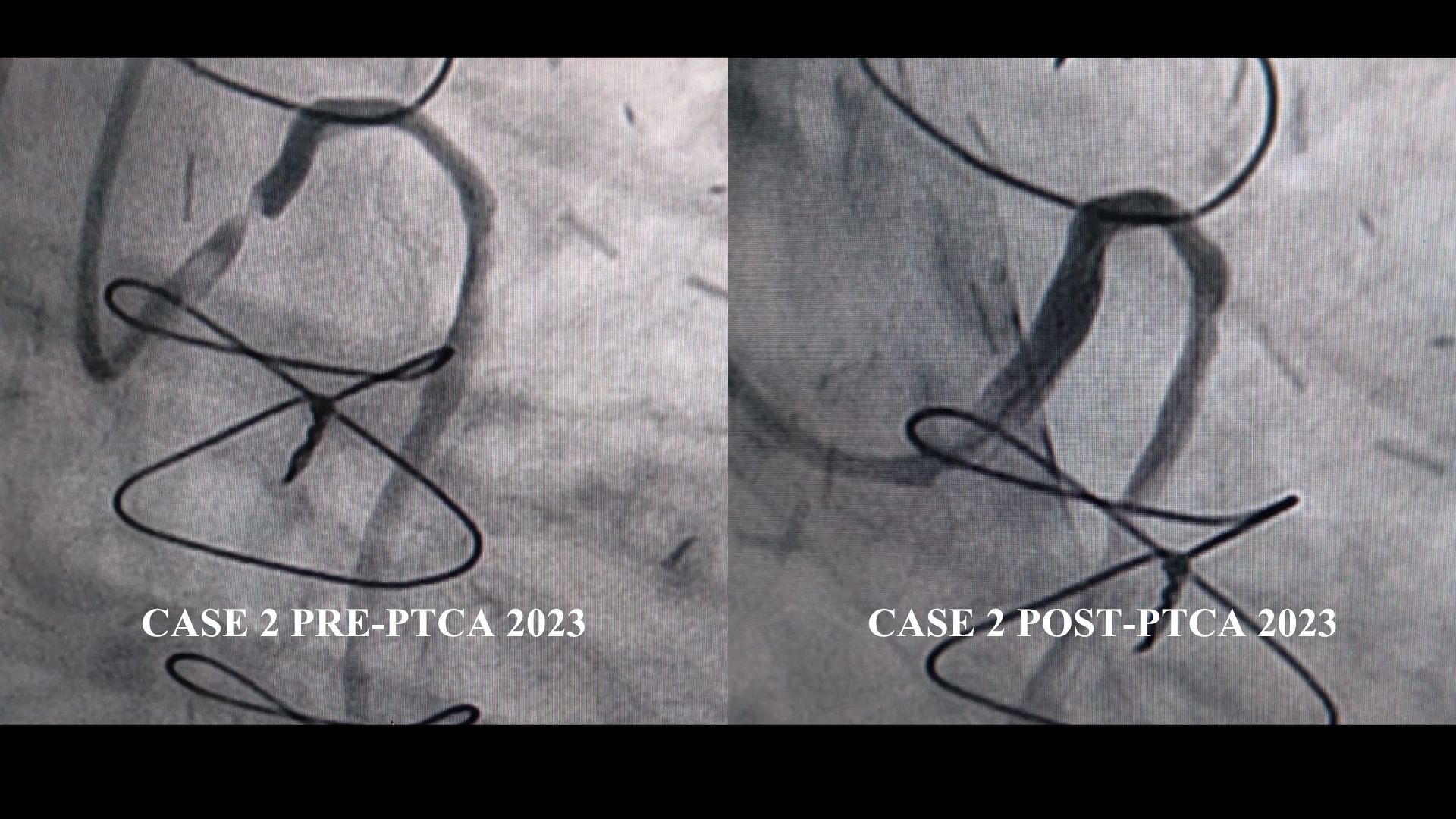
Case 1 – 72yr male CB presented with exertional chest pain for 15 days. Past history: NIDDM, HT. CABG in 2005 with pedicle LIMA–LAD, pedicle RIMA–RCA, and radial–OM. In 2019, due to unstable angina, he underwent PTCA to focal radial graft stenosis; other grafts were patent. Case 2 – 82yr male DP presented with acute chest pain for 2 hrs. Past history: HT. CABG in 2003 with pedicle LIMA–LAD, free RIMA–RCA, SVG–OM. In 2023, he underwent PTCA for focal SVG stenosis; other grafts patent.
Relevant Test Results Prior to Catheterization
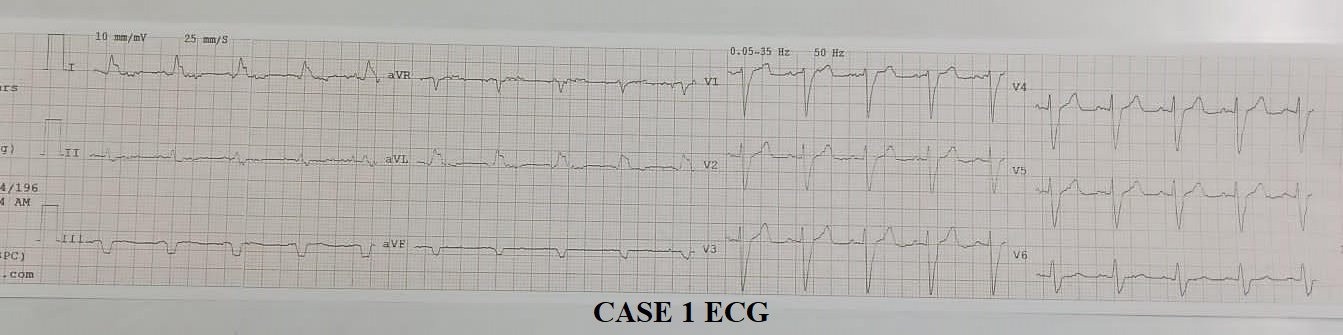
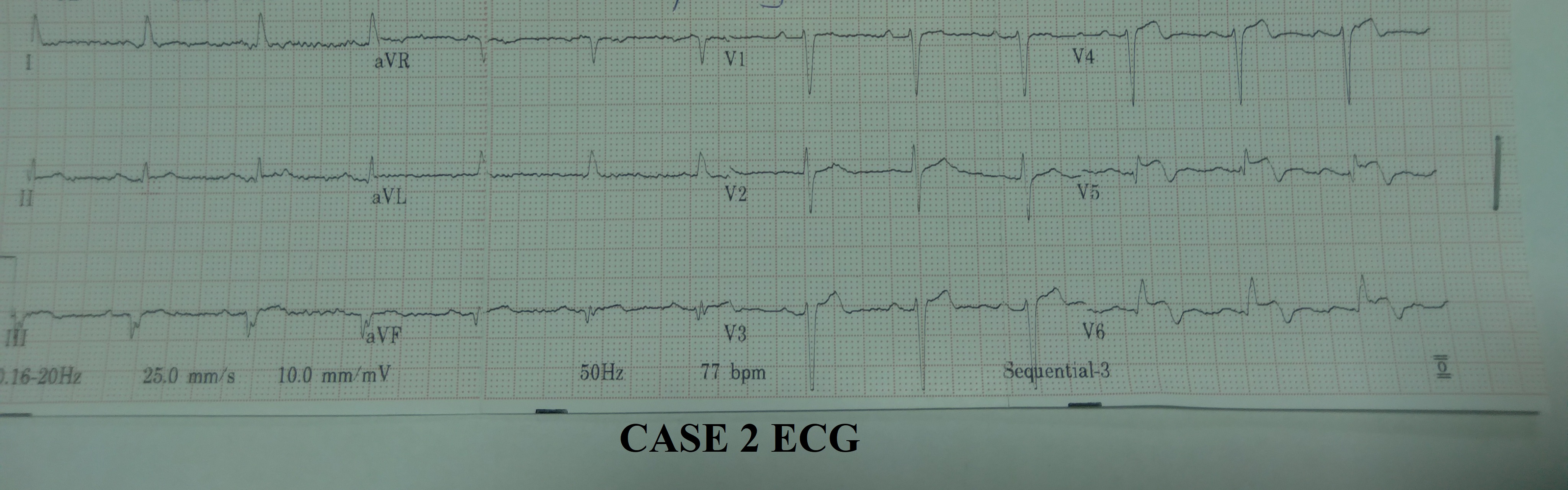
Case 1 – Clinical examination revealed HR 90/min, BP 126/78, ECG showed LBBB pattern. Chest X-ray was normal. 2D Echo: LVEF 42% with marked apicolateral hypokinesia and significant drop from previous study. Taken up for planned coronary angiography. Case 2 – Clinical examination revealed HR 70/min, BP 150/94, ECG showed ST elevation in V5–V6. 2D Echo: LVEF 45% with marked apical and anterolateral hypokinesia. Troponin I was elevated, hence he was taken for urgent angiography.
Relevant Catheterization Findings
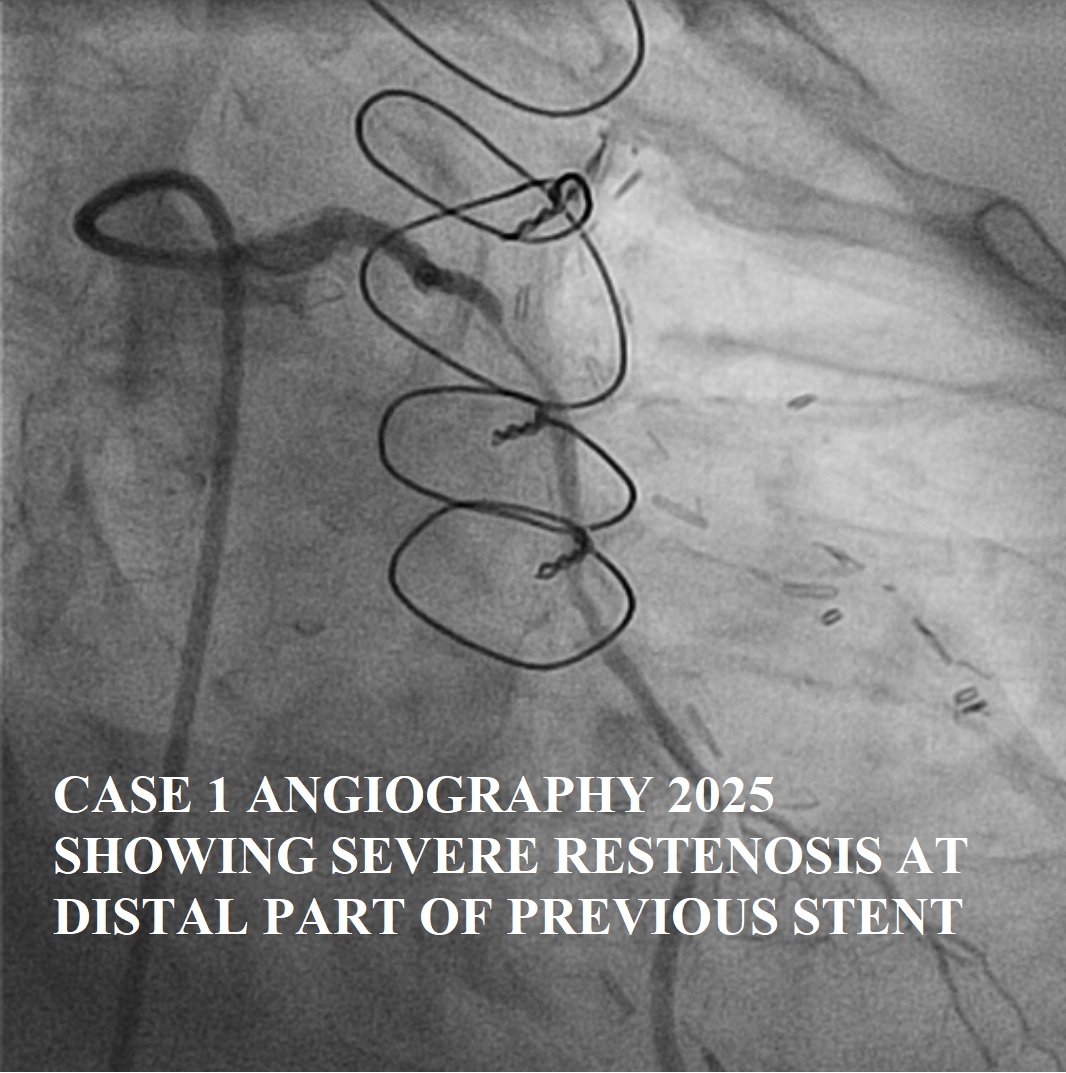
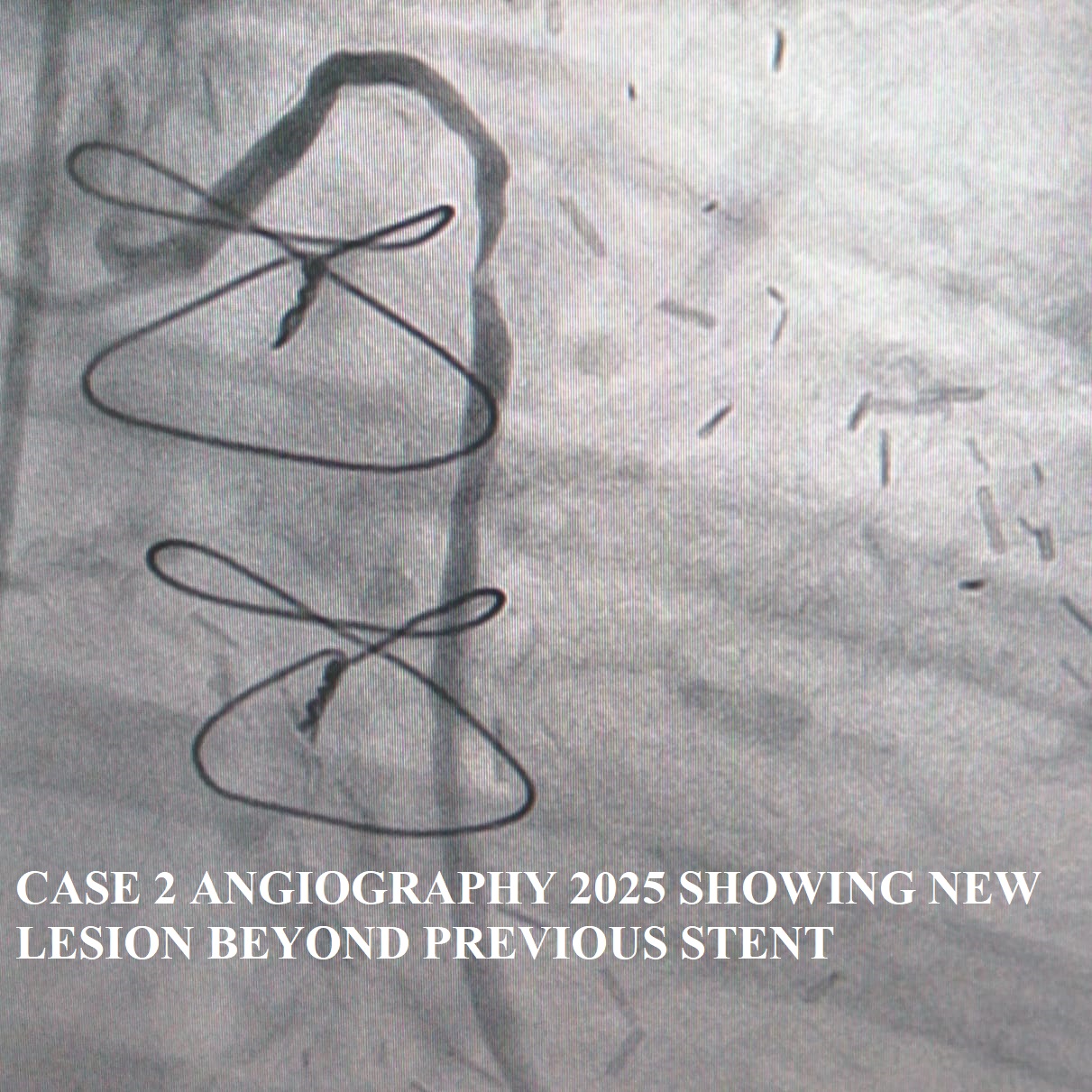
Case 1 – Angiography showed severe native left and right multivessel disease. Pedicle LIMA and RIMA grafts were patent with good distal flow. The free radial graft had a focal 90% stenosis at the distal edge of the prior stent. Case 2 – Severe native left and right multivessel disease was noted. LIMA–LAD graft patent with good flow. Free RIMA graft to RCA showed 40% proximal lesion with good distal flow. SVG–OM had a new 95% mid-graft stenosis beyond the previous stent without restenosis.
 1. CASE 1 ANGIOGRAPHY LOOP WITH CAPTION.mp4
1. CASE 1 ANGIOGRAPHY LOOP WITH CAPTION.mp4
2. CASE 2 ANGIOGRAPHY LOOP WITH CAPTION.mp4
Interventional Management
Procedural Step
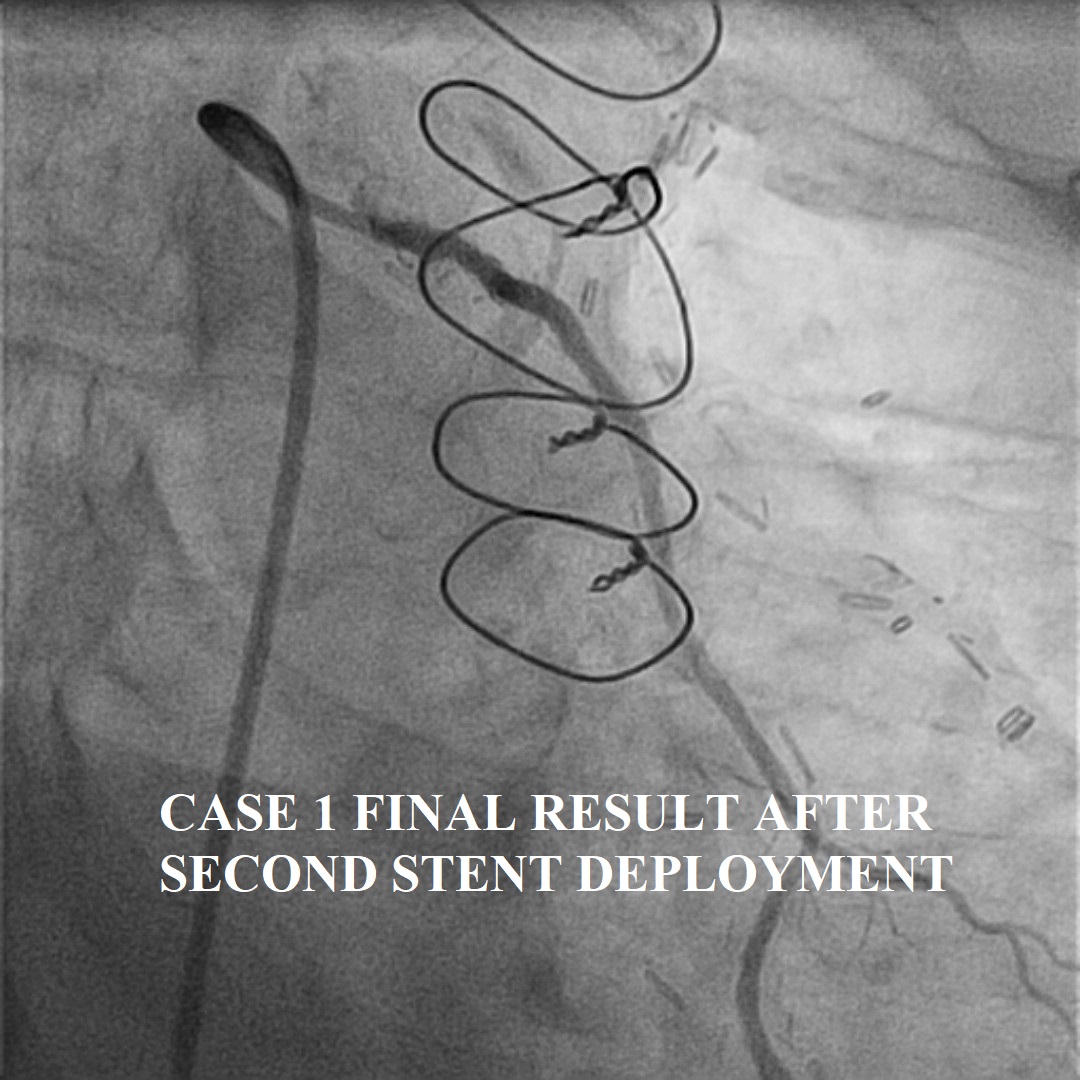
Case 1 – The free radial graft to OM was cannulated using a 6F 3DRC guiding catheter. The lesion was crossed with a TurnTrac wire and predilated with a 2.5× 15 NC Trek balloon. Due to the presence of a previous stent and graft angulation, tracking the new stent was challenging. Therefore, a 6F Guideliner extension catheter was advanced beyond the prior stent to facilitate delivery. A 2.75 × 28 mm Xience Alpine stent was deployed from the distal edge of the previous stent with adequate overlap, covering the entire lesion. TIMI III flow was achieved in the distal OM with excellent angiographic result. The patient had an uneventful recovery.
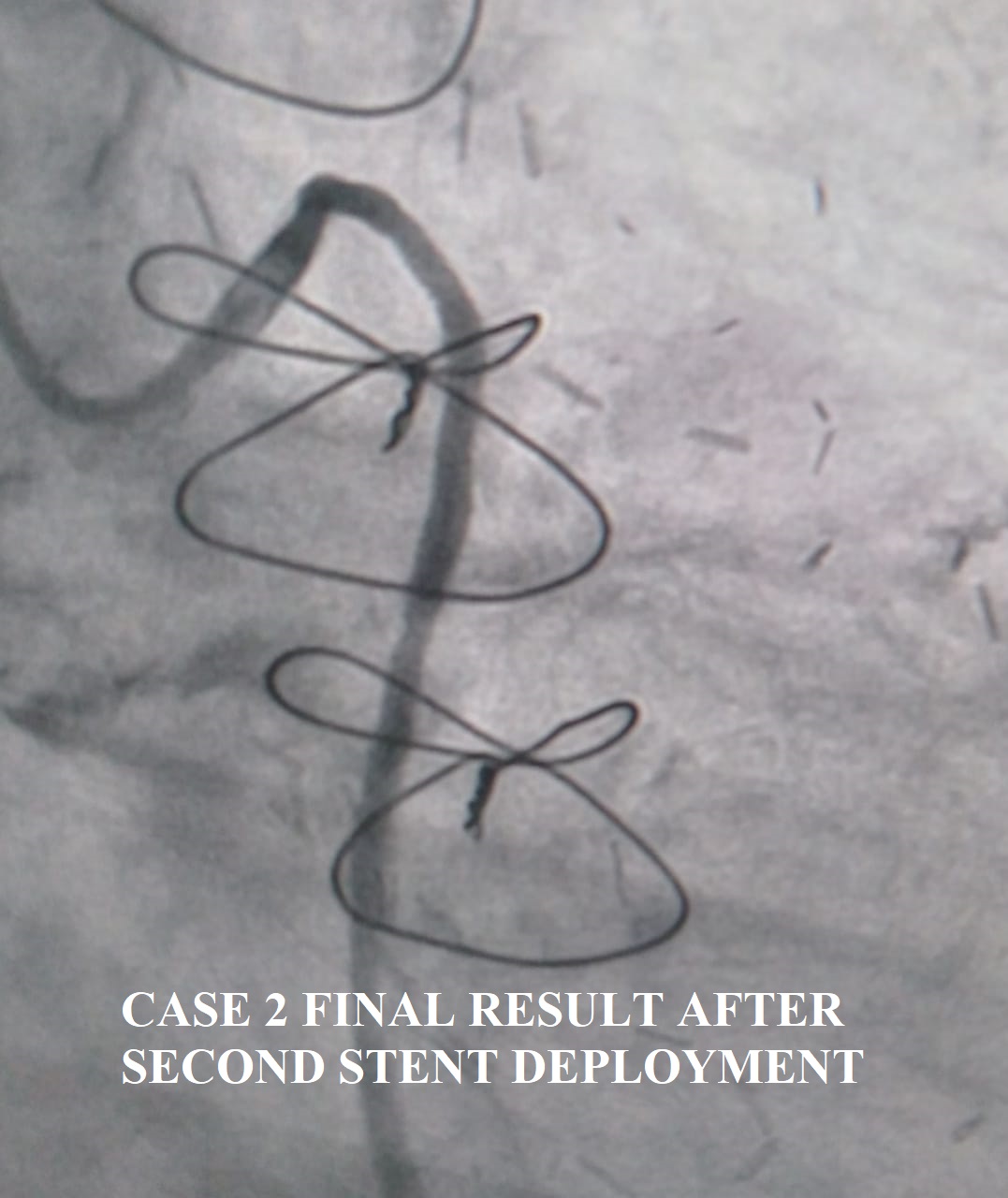
Case 2 – The SVG graft was cannulated using a 6F 3DRC guiding catheter. The lesion was crossed with a TurnTrac wire and predilated with a 2.5 × 15 NC Trek balloon. Subsequently, a 2.75 × 38 mm Xience Sierra stent was deployed beyond the distal edge of the previous stent, covering the entire lesion. TIMI III flow was achieved in the distal OM with good result. As this represented an acute ST-elevation myocardial infarction due to a recurrent SVG lesion, the patient received an intravenous bolus of Tirofiban followed by a 12-hour infusion. The recovery was uneventful.
2. CASE 1 GUIDELINER.mp4
3. CASE 1 FINAL RESULT with caption.mp4
4. CASE 2 FINAL RESULT WITH CAPTION.mp4
Case 2 – The SVG graft was cannulated using a 6F 3DRC guiding catheter. The lesion was crossed with a TurnTrac wire and predilated with a 2.5 × 15 NC Trek balloon. Subsequently, a 2.75 × 38 mm Xience Sierra stent was deployed beyond the distal edge of the previous stent, covering the entire lesion. TIMI III flow was achieved in the distal OM with good result. As this represented an acute ST-elevation myocardial infarction due to a recurrent SVG lesion, the patient received an intravenous bolus of Tirofiban followed by a 12-hour infusion. The recovery was uneventful.
Case Summary
In these challenging post CABG cases, there was recurrent stenosis in a single graft supplying a large OM territory. In Case 1 it was free radial graft and Case 2 it was saphenous vein graft. Challenges due to angulation of the grafts and a previously deployed stent need to be overcome. The 3DRC guiding catheter due its unique shape, is useful to selectively cannulate free grafts supplying OM which arise higher from the aorta. In Case 1, an additional guide extension catheter made it possible to negotiate the previous stent and curve of the graft. In Case 2 of a vein graft with STEMI, adjuvant tirofiban therapy was used due high thrombus load. Strict LDL control is key to prevent recurrence.