Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251024_001
Use of Resorbable Magnesium Scaffold on a Vulnerable Plaque and Restudy Coronary Angiogram in 6 months by Optical Coherence Tomography and Novel Angiographic-Based Radial Wall Strain
By Hang Long Li, Jeffrey Chun Yin Lee, Lap Tin Lam
Presenter
Hang Long Li
Authors
Hang Long Li1, Jeffrey Chun Yin Lee2, Lap Tin Lam2
Affiliation
Queen Mary Hospital, Hong Kong, China1, Grantham Hospital, Hong Kong, China2
View Study Report
CASE20251024_001
Coronary - Imaging & Physiology - Angiography/QCA
Use of Resorbable Magnesium Scaffold on a Vulnerable Plaque and Restudy Coronary Angiogram in 6 months by Optical Coherence Tomography and Novel Angiographic-Based Radial Wall Strain
Hang Long Li1, Jeffrey Chun Yin Lee2, Lap Tin Lam2
Queen Mary Hospital, Hong Kong, China1, Grantham Hospital, Hong Kong, China2
Clinical Information
Relevant Clinical History and Physical Exam
Mr. CWL is a 74-year-old male chronic smoker (> 50 pack-year). He has a long history of hyperlipidemia. He presented to the cardiology unit with central chest pain worse on exertion. Physical examination is unremarkable.

Relevant Test Results Prior to Catheterization
Computed Tomography (CT)-coronary angiogram revealed calcium score of 236, moderate atherosclerotic disease affecting all three coronary arteries, with severe stenosis at distal left circumflex artery (LCX). Electrocardiogram was unremarkable.
Relevant Catheterization Findings
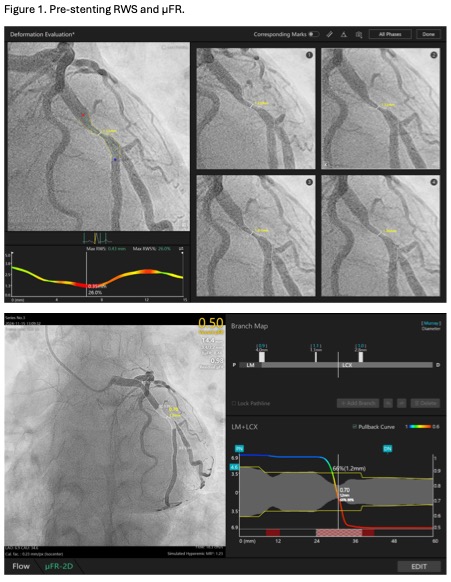
Coronary angiogram showed 90% stenosis of mid-LCX (Video 1). The maximum radial wall strain (RWS) was 26%, reflecting significant plaque vulnerability (>12%). Murray law-based quantitative flow ratio analysis (μFR) was 0.50 (Figure 1), reflecting functional significance (<0.80). Optical coherence tomography (OCT) showed fibroatheroma with lipid arc of 270 degrees with mild calcification (Video 2). Overall, the findings were consistent with vulnerable plaque at mLCx.
 Video 1.mp4
Video 1.mp4
Video 2.mp4
Video 3.mp4
Interventional Management
Procedural Step
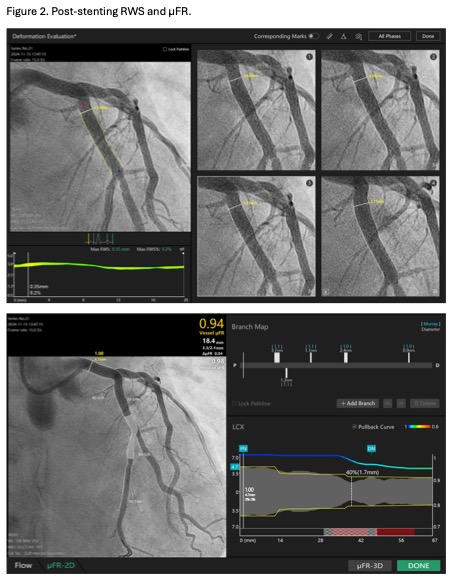
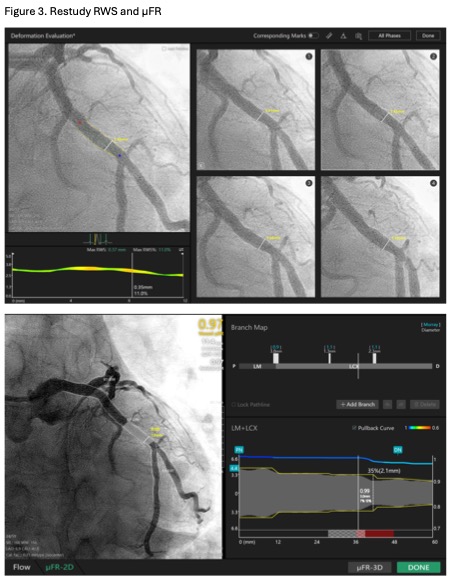
A 6Fr EBU 3.5 guiding catheter was engaged into the left main using right radial access. Distal LCX was wired using Rinato. Pre-dilatation was done using a 4.0/15 NC Scoreflex scoring balloon. Freesolve® 4.0/18 was implanted at 10atm. Post-dilatation was done using 4.5/15 Pantera Neo balloon. Results including stent expansion were excellent based on angiogram (Video 3) and OCT (Video 4). The post procedure RWS and μFR were 9.2% and 0.94, respectively (Figure 2).Six months later, we performed a restudy coronary angiogram for this patient, showing patent mLCX (Video 5), completely degraded resorbable scaffold and resolution of the vulnerable plaque on OCT (Video 6). The RWS and μFR were 0.37mm (11%) and 0.97, respectively (Figure 3). The patient remained asymptomatic.
Video 4.mp4
Video 5.mp4
Video 6.mp4
Case Summary
This case shows that vulnerable plaque (1) can be evaluated using novel indices including RWS/μFR and (2) can be managed using resorbable magnesium scaffold. Restudy angiogram revealed patent vessel, completely degraded resorbable scaffold, sustainably excellent OCT results, and improvement in RWS (26% to 11%) and μFR (0.50 to 0.97).Resorbable magnesium scaffold “leaves nothing behind” and has previously shown to be safe. It represents an appealing potential treatment for vulnerable plaque. Meanwhile, angiographic-based RWS has the advantages of detecting plaque vulnerability without the need of invasive coronary wire as well as the ability to provide functional assessment.