Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251022_004
Lost and Found: Left Main in STEMI
By Hing Yin Wilson Lam
Presenter
Hing Yin Wilson Lam
Authors
Hing Yin Wilson Lam1
Affiliation
Yan Chai Hospital, Hong Kong, China1
View Study Report
CASE20251022_004
Coronary - ACS/AMI
Lost and Found: Left Main in STEMI
Hing Yin Wilson Lam1
Yan Chai Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
71-year-old gentleman with a history of diabetes, hypertension, and hyperlipidemia presented with one day of chest pain. He was in cardiogenic shock, requiring high-flow oxygen support via a non-rebreathing mask to maintain saturation. He remained hemodynamically borderline, with a systolic blood pressure of 100-110 mmHg.
Relevant Test Results Prior to Catheterization
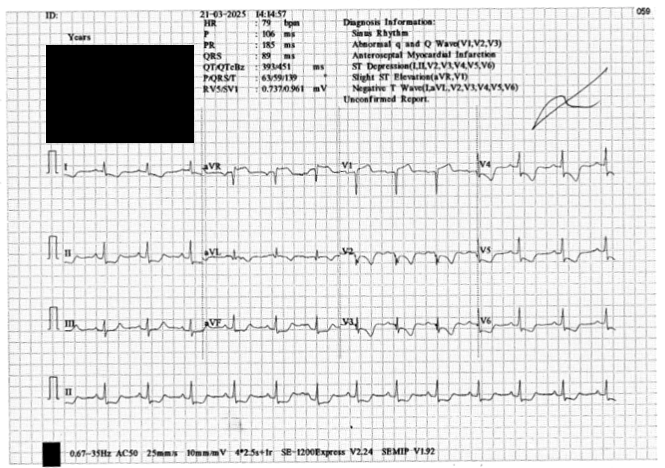
The admission ECG demonstrated ST-elevation in aVR with diffuse ST-depression across the precordial and inferior leads, suspicious for left main coronary occlusion. Bedside echocardiogram showed severe diffuse apical and anterior hypokinesia and a severely impaired left ventricular ejection fraction (LVEF) estimated at 20%.
Relevant Catheterization Findings

Interventional Management
Procedural Step
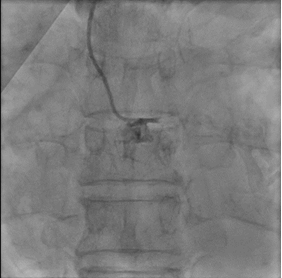
As patient is having cardiogenic shock from a LM occlusion and refusal of CABG, a high-risk, mechanically-supported PCI was undertaken. An IABP was inserted via the left femoral artery for hemodynamic support.Right femoral artery approach. 7Fr EBU 3.5 Guide. LAD and LCx were wired with microcatheter support. 2.0 balloon was used to predilate the LM-LAD lesion, TIMI 3 flow restored.IVUS was performed, showing heavily calcified plaque throughout the LM and LAD. Based on IVUS sizing (LM: 4.5mm, pLAD: 4.0mm), predilation with NC balloons followed by Intravascular Lithotripsy (IVL) with a 3.0 Shockwave balloon for 70 cycles were performed.A 2.75/40mm DES was placed in the mid-LAD and a 3.5/24mm DES was deployed from the ostial LM into the proximal LAD. POT in the LM using a 4.5 NC balloon, followed by post-dilation of the proximal LAD with a 4.0 NC balloon.Post-angiography revealed a jailed D1 with TIMI 0 flow. Rewiring to D1 was reattempted successfully with a CTO wire. Switched back to workhorse wire, dotted and predilated with 1.5 semi-compliant balloon. However IVUS showed wire likely true-false-true with ostial D1 in subintimal. Decided not to further intervene on D1.Final IVUS showed satisfactory results. Angiogram after adenosine showed regained flow in D1, TIMI 3 flow in both LAD and D1. Patient remained hemodynamically stable on IABP support post-procedure.



Case Summary
This case demonstrates the successful application of an imaging-guided strategy in a patient with cardiogenic shock from an occluded left main. The primary challenge was severe calcification, which was effectively managed with intravascular lithotripsy (IVL) following IVUS assessment. With mechanical support, IVL, and IVUS, high-risk PCI can be a safe and effective revascularization strategy for LM STEMI.