Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251022_003
Successful Salvage of Fulminant Influenza a Perimyocarditis in a 47-Year-Old Patient: Overcoming Severe Cardiogenic Shock With Combined ECMO and IABP Strategy
By Wichid Thirakraisri, Wittawat Wattanasiriporn, Chatchai Pitakrattanachai
Presenter
Wichid Thirakraisri
Authors
Wichid Thirakraisri1, Wittawat Wattanasiriporn1, Chatchai Pitakrattanachai1
Affiliation
Rajavithi Hospital, Thailand1
View Study Report
CASE20251022_003
Heart Failure - Cardiogenic Shock
Successful Salvage of Fulminant Influenza a Perimyocarditis in a 47-Year-Old Patient: Overcoming Severe Cardiogenic Shock With Combined ECMO and IABP Strategy
Wichid Thirakraisri1, Wittawat Wattanasiriporn1, Chatchai Pitakrattanachai1
Rajavithi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A 47-year-old Thai female with no prior medical history presented with a 6-day history of upper respiratory symptoms (cough, rhinorrhea, fever) followed by progressive exertional dyspnea over 24 hours. She denied chest pain, orthopnea, or paroxysmal nocturnal dyspnea.Vital signs were abnormal: BP 80/50 mmHg, HR 110 bpm, RR 28/min, temperature 37.8°C, SpO2 92% on room air. Physical examination revealed normal heart sounds without murmurs, but bilateral fine crepitations.
Relevant Test Results Prior to Catheterization
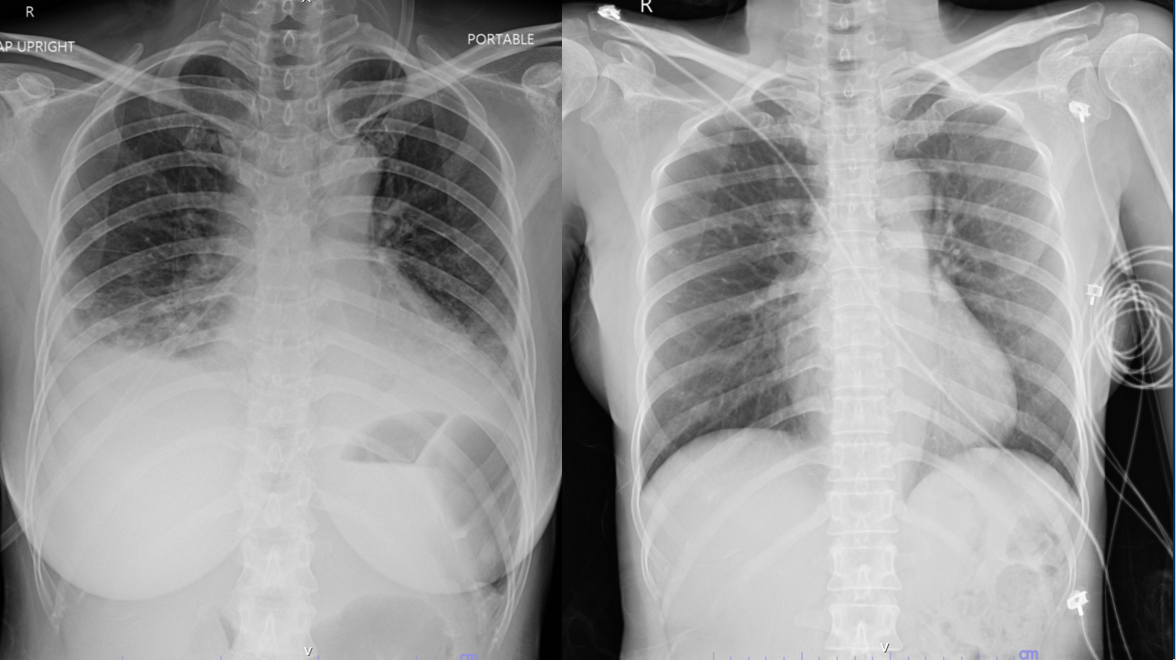
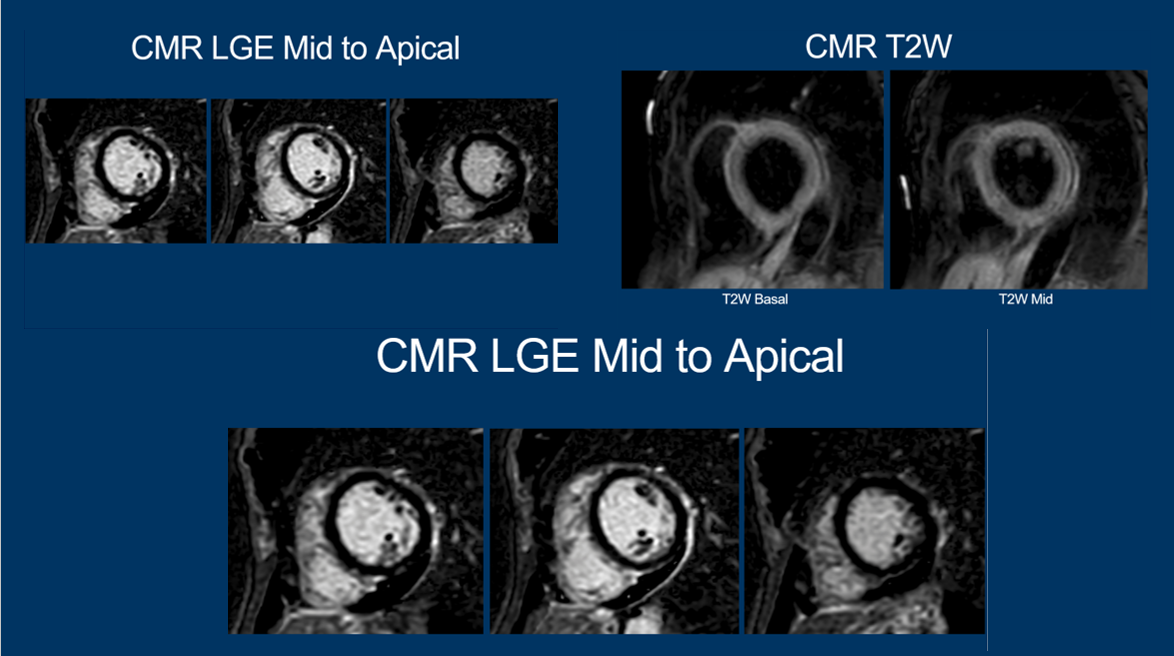
Initial ECG showed sinus tachycardia with low voltage QRS and minimal ST elevation in inferior leads. Chest X-ray revealed cardiomegaly, bilateral infiltrates, and pleural effusions consistent with acute heart failure.Laboratory findings: troponin I 1,400 ng/L, NT-proBNP 19,903 pg/mL, lactate 5.7 mmol/L, AST 483 U/L, ALT 611 U/L, hsCRP 6.31 mg/dL, Echocardiography showed LVEF 29.4% with global hypokinesia, impaired RV function (TAPSE 12 mm), and mild pericardial effusion (0.4 cm).
Relevant Catheterization Findings
Emergencycoronary angiography excluded obstructive coronary artery disease, confirmingnormal coronary anatomy.The clinical presentation, imaging findings, elevated biomarkers, and confirmed influenza infection established the diagnosis of fulminant Influenza A perimyocarditis complicated by severe cardiogenic shock, classified as SCAI Stage D and INTERMACS Profile 2 (progressive decline despite inotropic support).
Interventional Management
Procedural Step
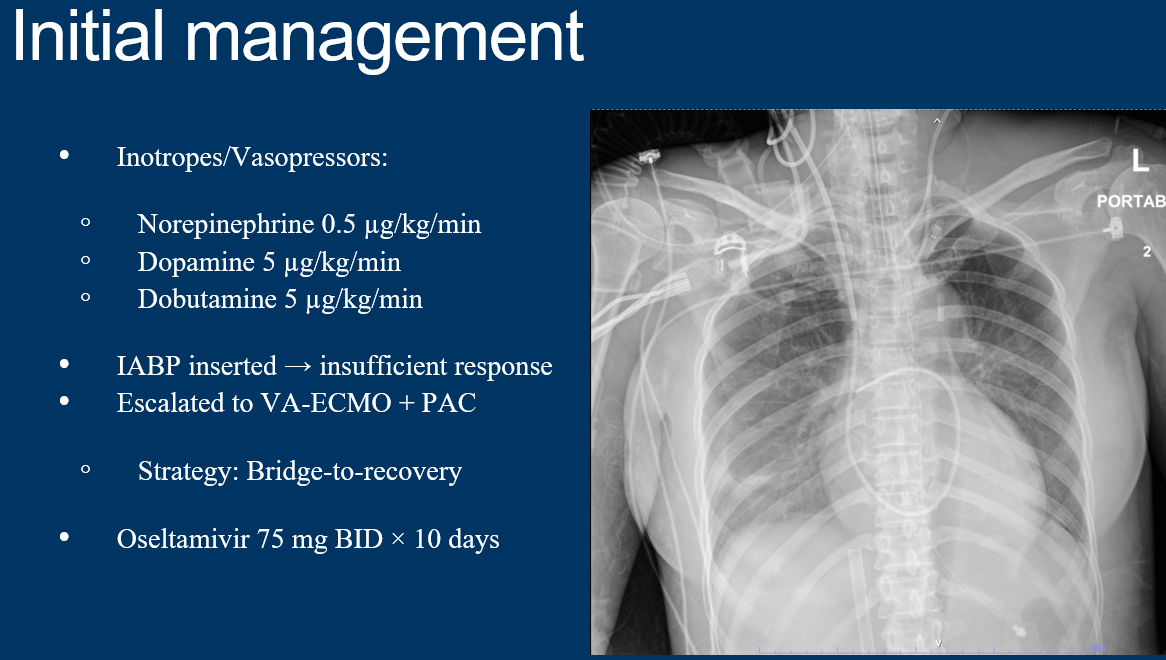
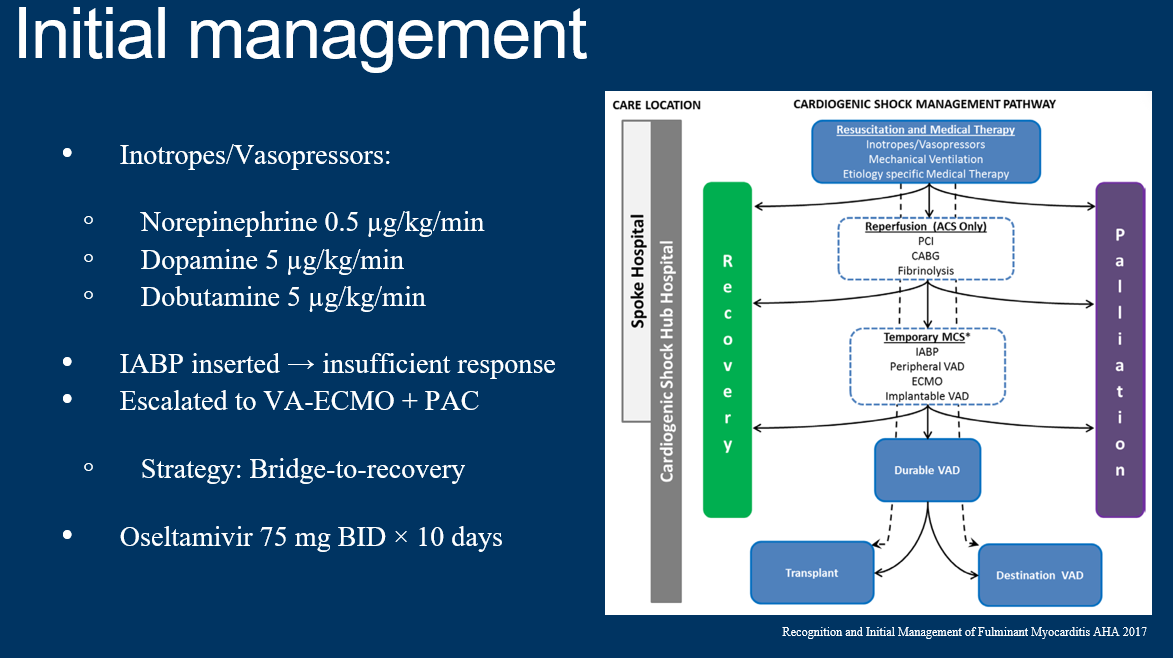
Despite maximum medical therapy with high-dose catecholamines, the patient continued to demonstrate signs of progressive hemodynamic deterioration with persistent hypotension, worsening metabolic acidosis, and clinical evidence of end-organ hypoperfusion including decreased urine output and altered mental status. Given the inadequate response to pharmacological support, the decision was made to escalate to mechanical circulatory support. An intra-aortic balloon pump (IABP) was initially inserted via the right femoral artery under fluoroscopic guidance and positioned in the descending thoracic aorta with the tip 2 cm distal to the left subclavian artery. The balloon was set to 1:1 counterpulsation. However, despite optimal IABP function with appropriate augmentation of diastolic pressure and reduction in afterload, hemodynamic parameters failed to improve significantly, with persistent hypotension (mean arterial pressure <60 mmHg), elevated lactate, and ongoing requirement for high-dose inotropes. Given the insufficient response to IABP alone and recognizing the critical nature of the presentation with imminent risk of multi-organ failure and cardiac arrest, the multidisciplinary team made the decision to urgently initiate veno-arterial extracorporeal membrane oxygenation (VA-ECMO) as a bridge-to-recovery strategy within 6 hours of initial presentation. Simultaneously, a PA catheter was inserted via the right internal jugular vein for comprehensivehemodynamic monitoring.
Case Summary
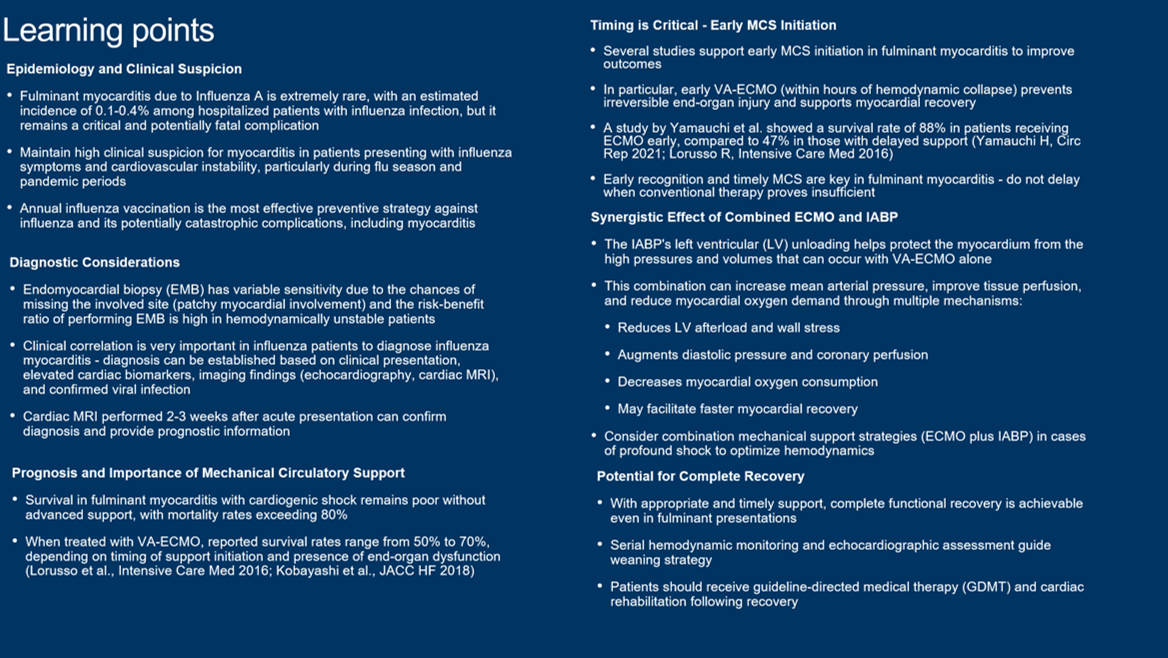
This case demonstrates the critical importance of early mechanical circulatory support in fulminant viral myocarditis. Influenza A myocarditis, though rare (0.1-0.4% of hospitalized influenza patients), carries high mortality without aggressive intervention. Prompt escalation to combined VA-ECMO and IABP within 6 hours prevented irreversible organ damage and facilitated complete cardiac recovery. The synergistic effect of ECMO and IABP (offering LV unloading) likely contributed to the short 6-day support duration. This case reinforces that early recognition and timely MCS are lifesaving in fulminant myocarditis presenting with cardiogenic shock.