Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251022_002
Ellis Class III Coronary Perforation During Intravascular Lithotripsy-Assisted Right Coronary Intervention
By Yu-Ching Chien, Yen-Lien Chou
Presenter
Yu-Ching Chien
Authors
Yu-Ching Chien1, Yen-Lien Chou2
Affiliation
Division of Cardiology, Songshan Branch of Tri-Service General Hospital, Taiwan1, Division of Cardiology, Tri-Service General Hospital, Taiwan2
View Study Report
CASE20251022_002
Coronary - Complication Management
Ellis Class III Coronary Perforation During Intravascular Lithotripsy-Assisted Right Coronary Intervention
Yu-Ching Chien1, Yen-Lien Chou2
Division of Cardiology, Songshan Branch of Tri-Service General Hospital, Taiwan1, Division of Cardiology, Tri-Service General Hospital, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
A 77-year-old man with hypertension, dyslipidemia, and previous subacute cerebral infarction presented with exertional dyspnea for two months. He had known triple-vessel coronary artery disease with prior PCI to the LCX. Physical examination revealed clear lungs, regular heartbeat without murmurs, and no peripheral edema. He was admitted for elective CAG and possible PCI for residual LAD and RCA stenoses.
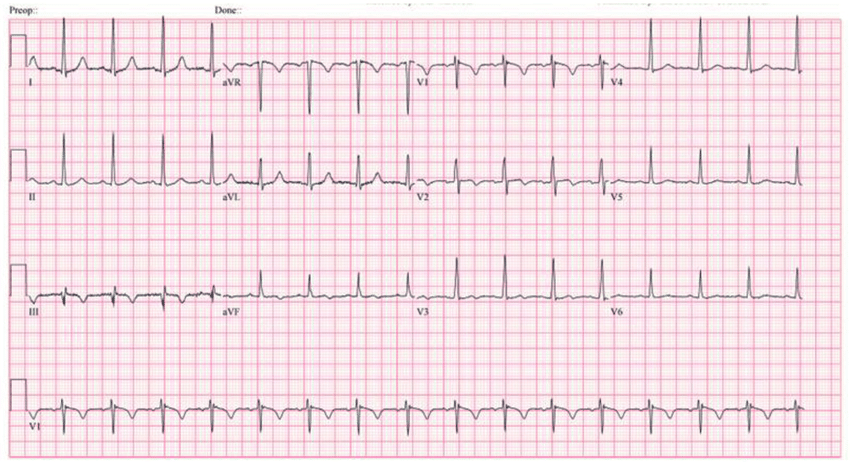
Relevant Test Results Prior to Catheterization
Myocardial perfusion imaging revealed partially reversible severe hypoperfusion over the lateral and inferior walls of the left ventricle. Echocardiography showed preserved left ventricular systolic function with an ejection fraction of 64%, mild to moderate aortic regurgitation, and mild mitral and tricuspid regurgitation. Baseline laboratory data demonstrated normal renal function (Cr 1.1 mg/dL), normal electrolytes. Chest X-ray revealed no significant infiltrations.
Relevant Catheterization Findings
Coronary angiography showed a patent left main artery. The LAD had luminal irregularity with diffuse 70–90% stenosis from proximal to distal segments (Medina 1,0,1) involving the first diagonal branch and 70–80% tubular stenosis at the D1 ostium. The LCX showed prior stenting from proximal LCX to OM1 without in-stent restenosis and additional 50–60% stenosis at mid to distal segments. The RCA revealed diffuse eccentric 70–95% stenosis with severe calcification from proximal to distal segment.
 1.mp4
1.mp4
Interventional Management
Procedural Step
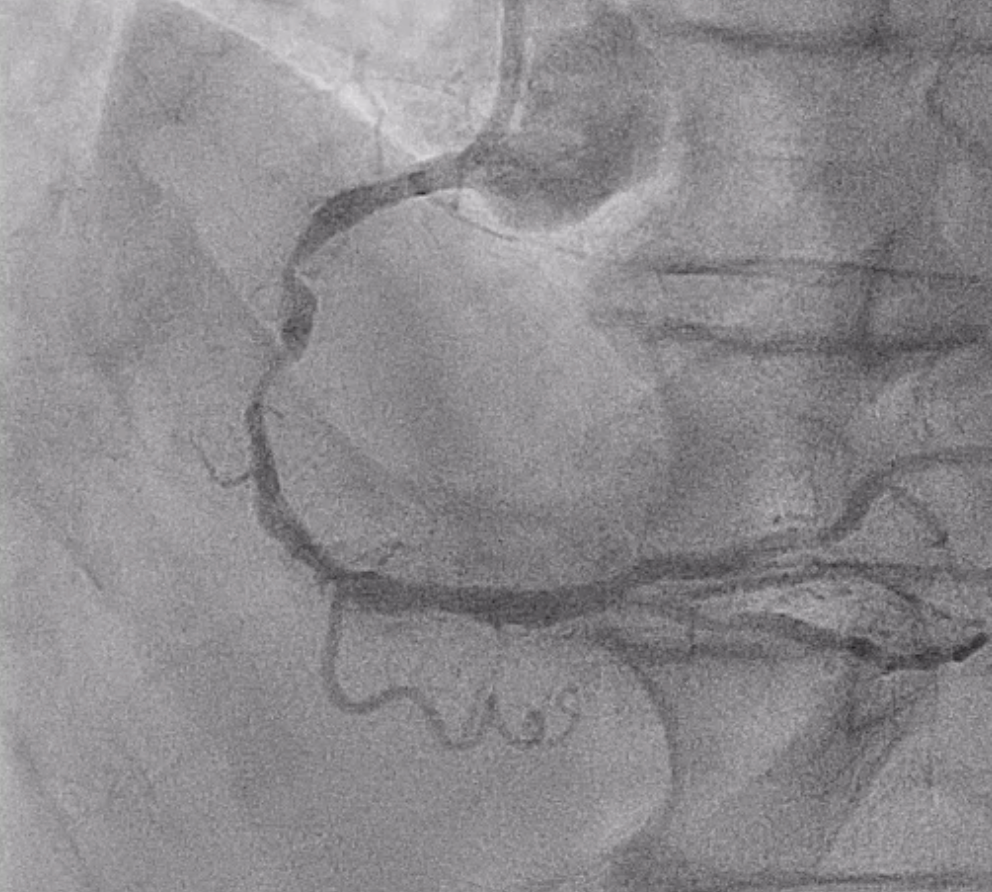
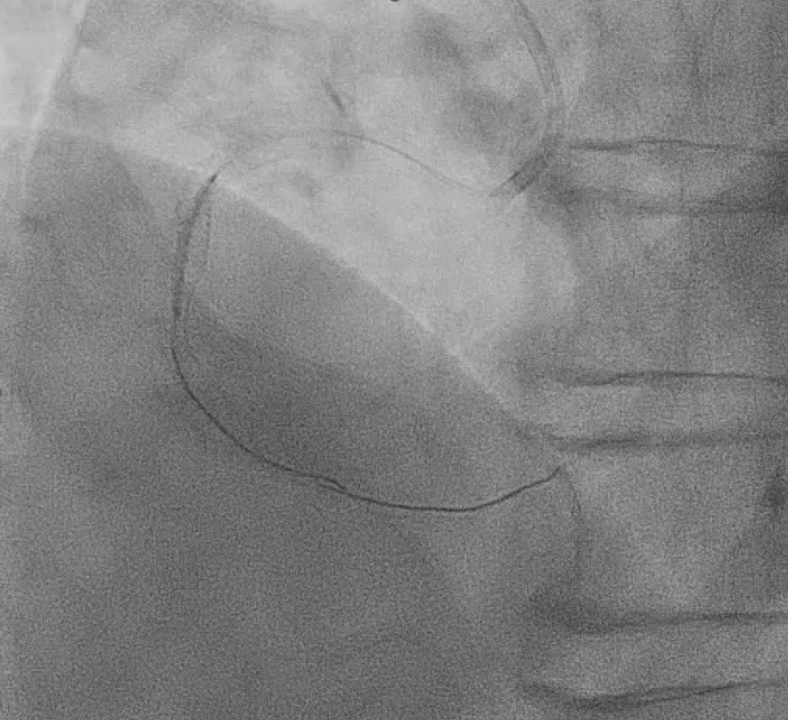
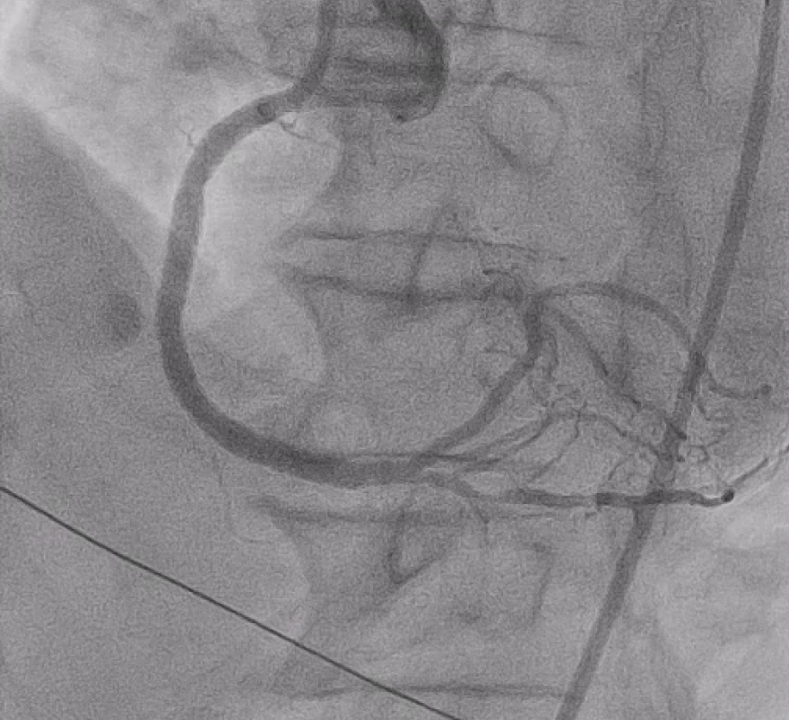
Right distal radial artery was used for access with a 6 Fr JR 3.5 guiding catheter. Anticoagulation was given to keep ACT >250 seconds and dual antiplatelet therapy was continued. A Runthrough wire crossed the diffusely calcified RCA lesion from proximal to distal. Sequential predilation with 2.0–3.0 mm non-compliant balloons was performed to assess vessel compliance.IVUS showed heavy concentric calcification with a minimal lumen area of 3.3 mm². Calcium modification was done using a 4.0 × 12 mm intravascular lithotripsy balloon with a total of 70 pulses, achieving good luminal expansion. Two drug-eluting stents were then implanted: 3.5 × 50 mm at mid–distal RCA and 4.0 × 24 mm at proximal–mid RCA, followed by high-pressure post-dilation up to 20 atm.After optimization, angiography revealed Ellis class II–III perforation at mid RCA. A 7 Fr system with Guideliner support was used for bailout. A 3.5 × 19 mm covered stent was deployed to seal the perforation, followed by additional dilation. Because of residual contrast leakage, another 3.5 × 16 mm covered stent was placed at proximal RCA, achieving complete sealing.Final IVUS confirmed good stent expansion and apposition. Angiography showed less than 30% residual stenosis with TIMI 3 flow.

Extra2.mp4
Graft1.mp4
SecondRoundPostGraft2.mp4
Case Summary
This case demonstrates the usefulness of intravascular lithotripsy (IVL) in modifying heavily calcified coronary lesions and emphasizes the importance of prompt management of complications. Although an Ellis class II–III perforation occurred after high-pressure post-dilation, immediate covered stent implantation effectively sealed the perforation and restored TIMI 3 flow. In similar cases, gradual balloon sizing, lower post-dilation pressure, and repeated imaging assessment during lesion preparation may help reduce the risk of vessel injury. This case highlights the balance between aggressive plaque modification and procedural safety in complex RCA interventions.