Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251022_001
Recurrent External Iliac Artery Stent Thrombosis Successfully Managed by Addressing Residual Superficial Femoral Artery Lesion in a 60-Year-Old Man
By Rie Aoyama, Yo Iwata, Shinichi Okino, Shigeru Fukuzawa
Presenter
Rie Aoyama
Authors
Rie Aoyama1, Yo Iwata1, Shinichi Okino1, Shigeru Fukuzawa1
Affiliation
Department of Cardiology, Heart and Vascular Institute Funabashi Municipal Medical Center, Japan1
View Study Report
CASE20251022_001
Endovascular - Iliac / SFA Intervention
Recurrent External Iliac Artery Stent Thrombosis Successfully Managed by Addressing Residual Superficial Femoral Artery Lesion in a 60-Year-Old Man
Rie Aoyama1, Yo Iwata1, Shinichi Okino1, Shigeru Fukuzawa1
Department of Cardiology, Heart and Vascular Institute Funabashi Municipal Medical Center, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A man in his early 60s presented with worsening intermittent claudication and new-onset rest pain in his left leg. He had experienced sudden pain during soccer six months earlier but was initially misdiagnosed as musculoskeletal. The symptoms did not improve with topical treatments such as pain relief patches, and he was referred to our hospital six months after onset. On examination, left femoral and pedal pulses were absent, while the right side was normal.

Relevant Test Results Prior to Catheterization
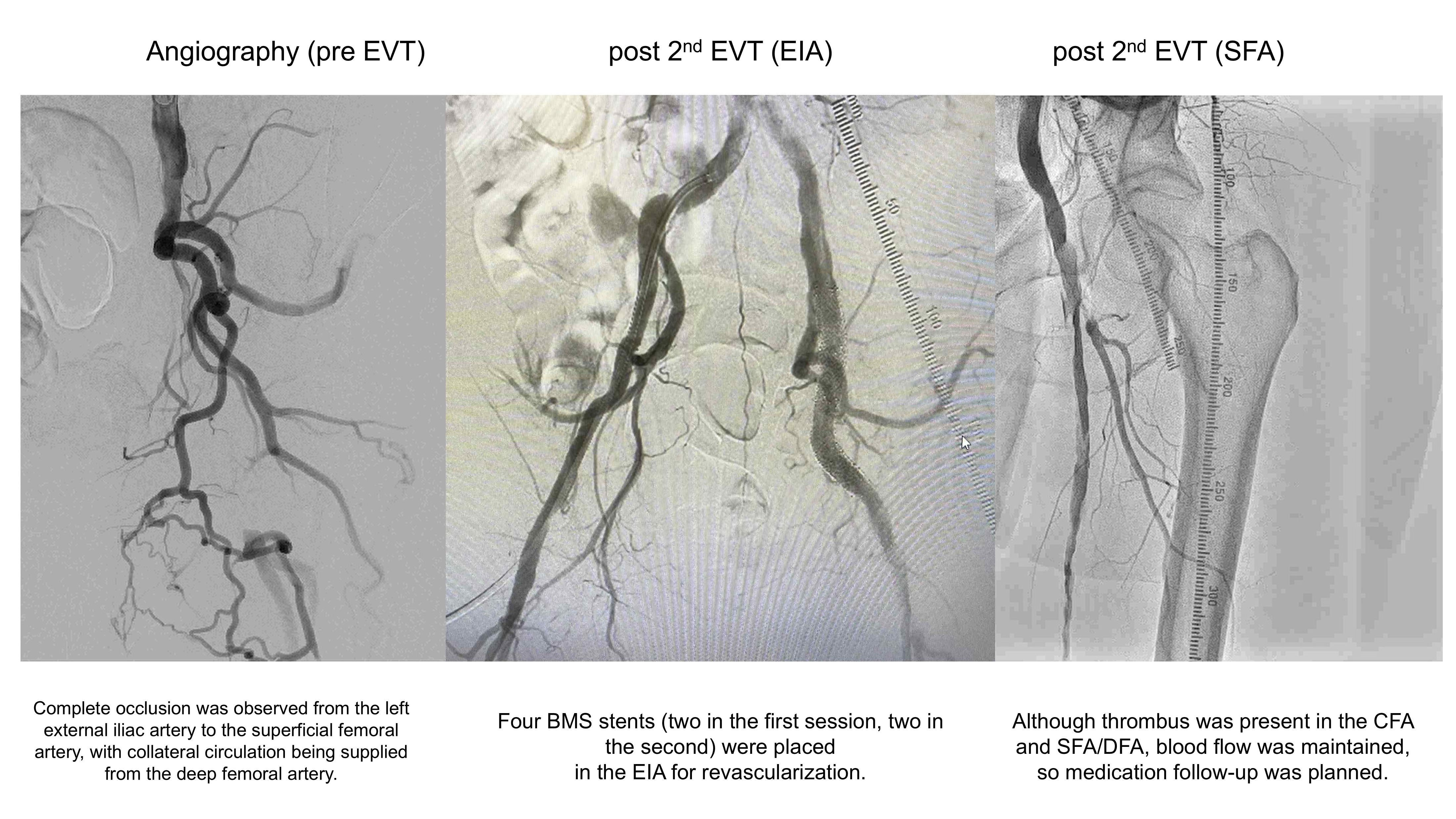
CT angiography showed total occlusion of the left external iliac artery (EIA) with preserved flow to the distal superficial femoral artery (SFA) via collaterals. Electrocardiography revealed a normal sinus rhythm without arrhythmia. Echocardiography was normal, and laboratory data showed no evidence of hypercoagulable disorder.
Relevant Catheterization Findings
Interventional Management
Procedural Step
First EVT: Via right femoralcrossover approach, total EIA occlusion was confirmed by angiography. Thrombusaspiration with a TVAC catheter (Nipro, Osaka, Japan) restored partial flow, and two bare-metalstents (BMS, Smart, Cordis, Miami Lakes, FL) were implanted in the EIA.Intravascular ultrasound (IVUS) demonstrated that the EIA lesion was thromboticrather than atherosclerotic. In addition, residual thrombus was detected in theproximal SFA, and POBA was performed for this segment.
Case Summary
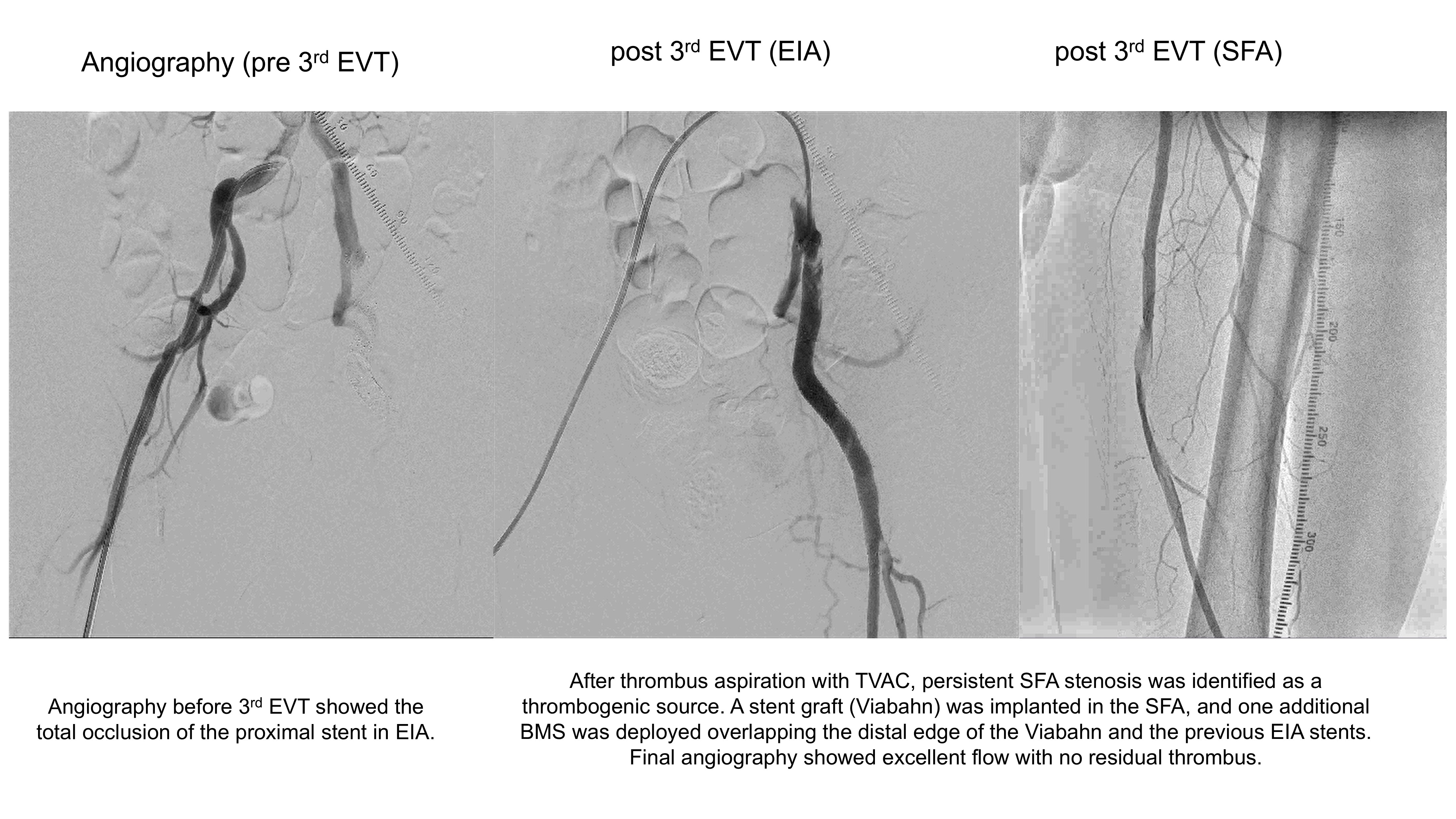
Repeatedstent thrombosis in the EIA was successfully managed by treating the residualSFA lesion, which had impaired runoff and promoted thrombosis. This caseunderscores the importance of addressing both inflow and outflow lesions fordurable revascularization outcomes in recurrent thrombotic iliac arterydisease.