Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251021_003
Scaling the Summit: Breaking Through a Blunt Ostial Left Anterior Descending Artery Chronic Total Occlusion in a Complex Coronary Bifurcation
By Christian Sunur, Chai Yih Tan, Kai Soon Liew, Prabahkar Subramaniam, Nancy Virginia, Saravanan Krishinan, Kantha Rao Narasamuloo, Dharmaraj Karthikesan
Presenter
Christian Sunur
Authors
Christian Sunur1, Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Nancy Virginia1, Saravanan Krishinan1, Kantha Rao Narasamuloo1, Dharmaraj Karthikesan1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1
View Study Report
CASE20251021_003
Coronary - Complex PCI - CTO
Scaling the Summit: Breaking Through a Blunt Ostial Left Anterior Descending Artery Chronic Total Occlusion in a Complex Coronary Bifurcation
Christian Sunur1, Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Nancy Virginia1, Saravanan Krishinan1, Kantha Rao Narasamuloo1, Dharmaraj Karthikesan1
Hospital Sultanah Bahiyah, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 69-year-old male with CCS class II angina despite optimal medical therapy and recurrent intradialytic hypotension. Risk factors include diabetes on insulin, hypertension, and end-stage renal failure on hemodialysis. He had a prior NSTEMI six months ago. Cardiovascular examination was unremarkable. CABG was recommended but refused.

 Diagnostic RCA.mp4
Diagnostic RCA.mp4
LCA RAO CAU.mp4
LCA spider.mp4
Relevant Test Results Prior to Catheterization
ECG showed normal sinus rhythm. Echocardiography revealed normal chambers, preserved systolic and diastolic function, and no valvular abnormalities. Laboratory testing demonstrated severely reduced renal function, with an estimated GFR of 8.3 mL/min/1.73 m².
Relevant Catheterization Findings
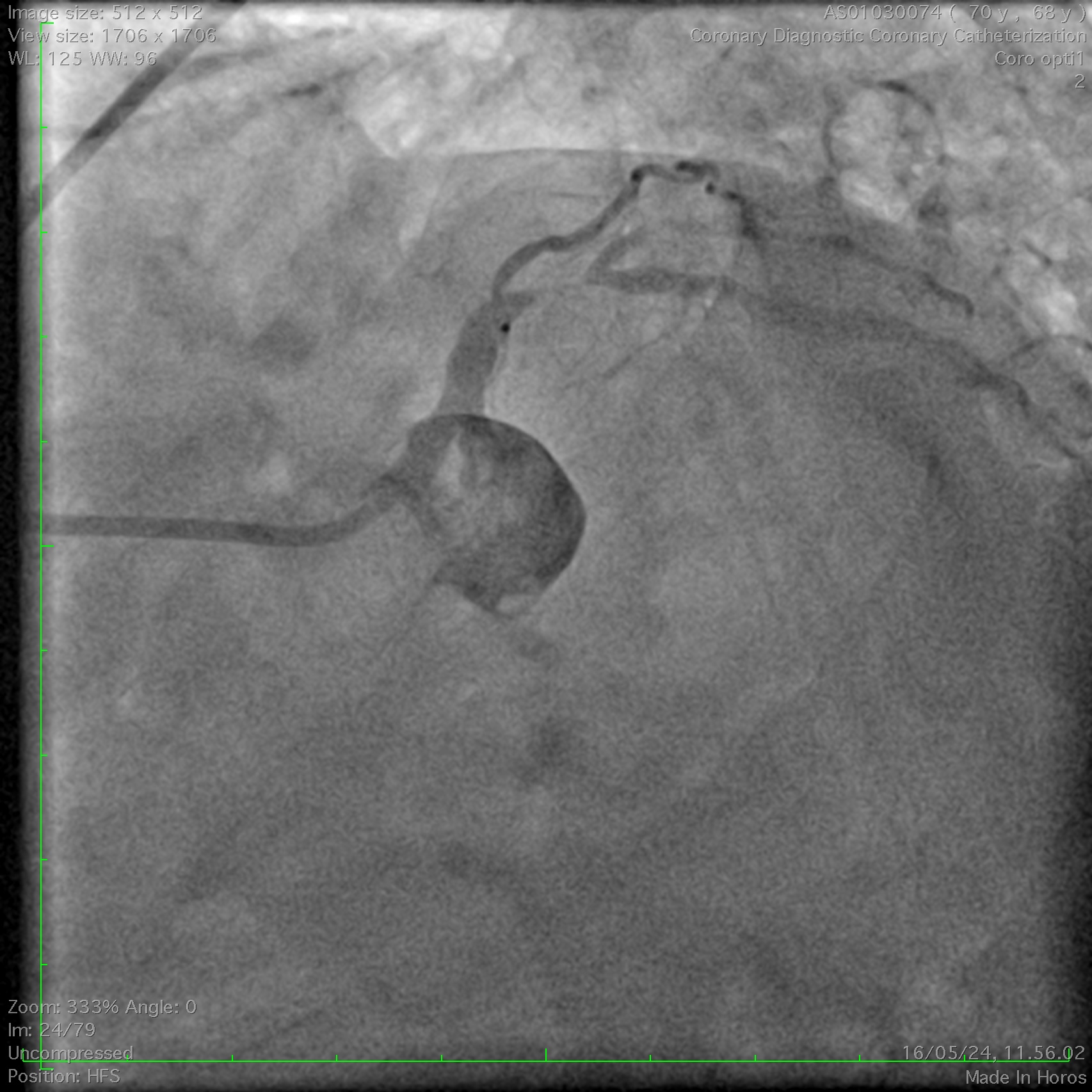
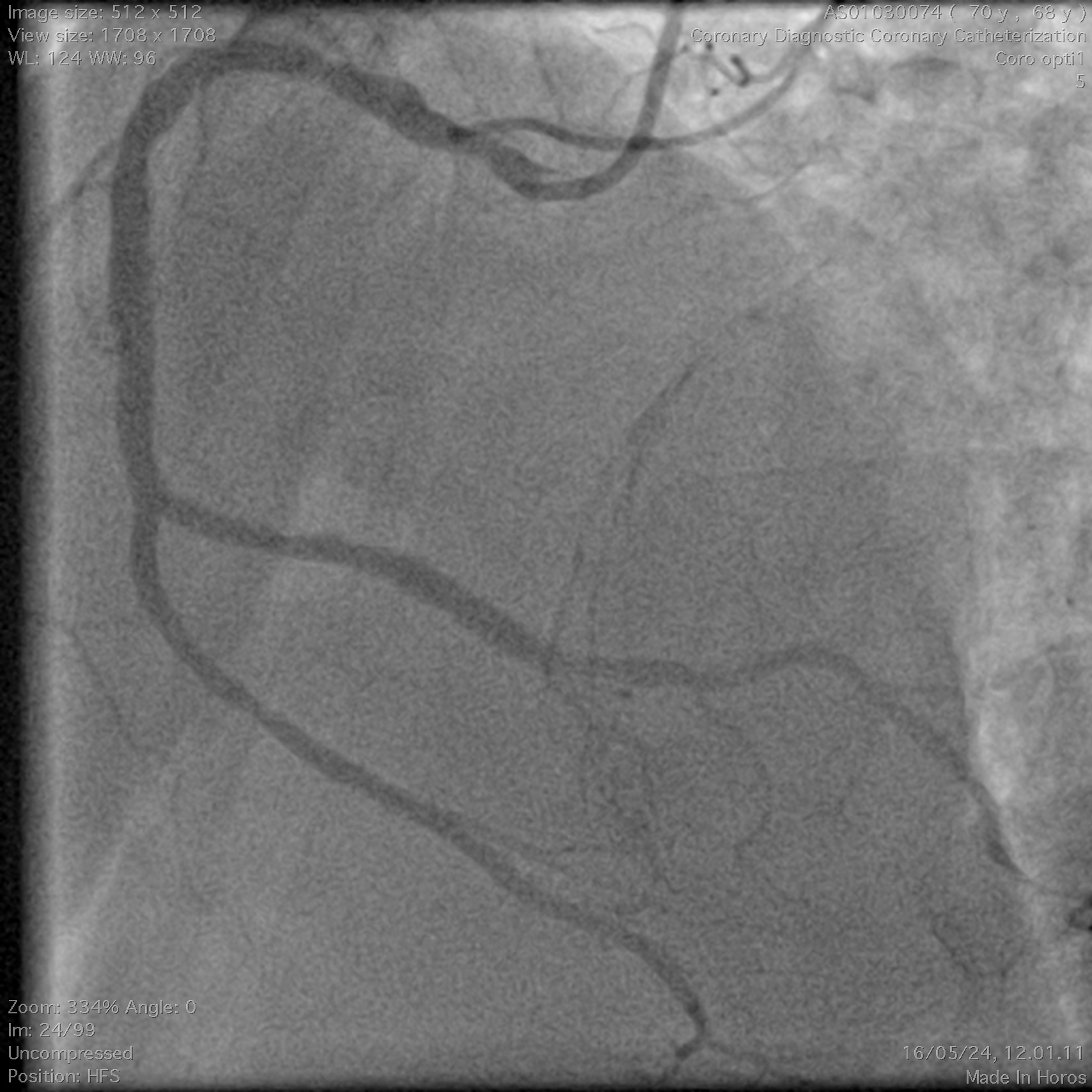
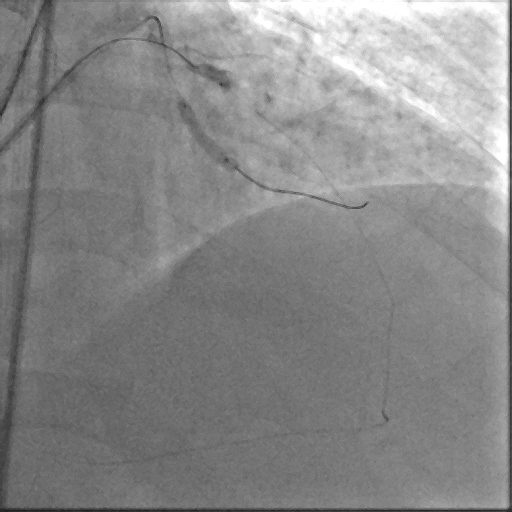
Coronary angiography demonstrated a right-dominant system with significant ostial LCx stenosis and a blunt ostial LAD chronic total occlusion, with a J-CTO score of 4. The RCA showed mild coronary disease and supplied collateral flow to the LAD territory, graded as Werner CC2.
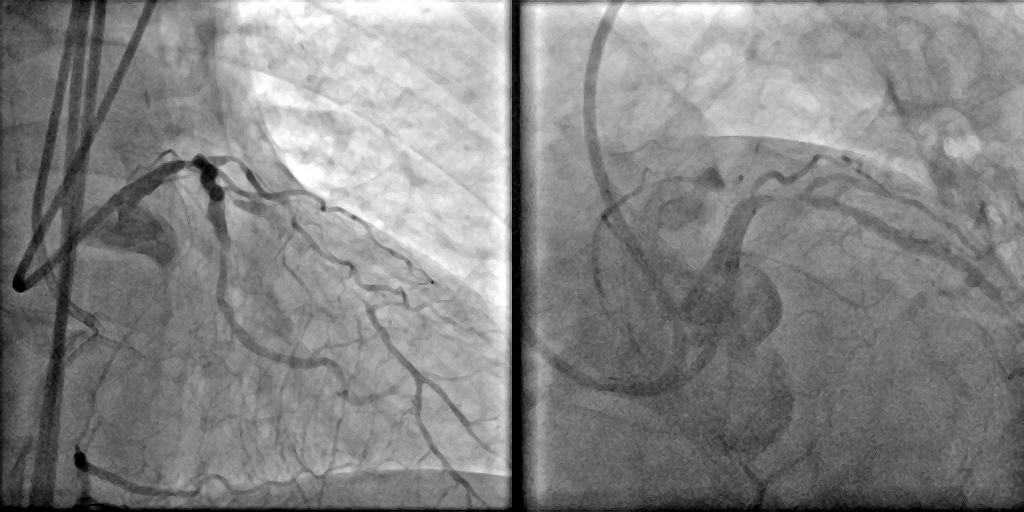
Bilateral injection Spider.mp4
Collateral Bilateral Injection.mp4
Interventional Management
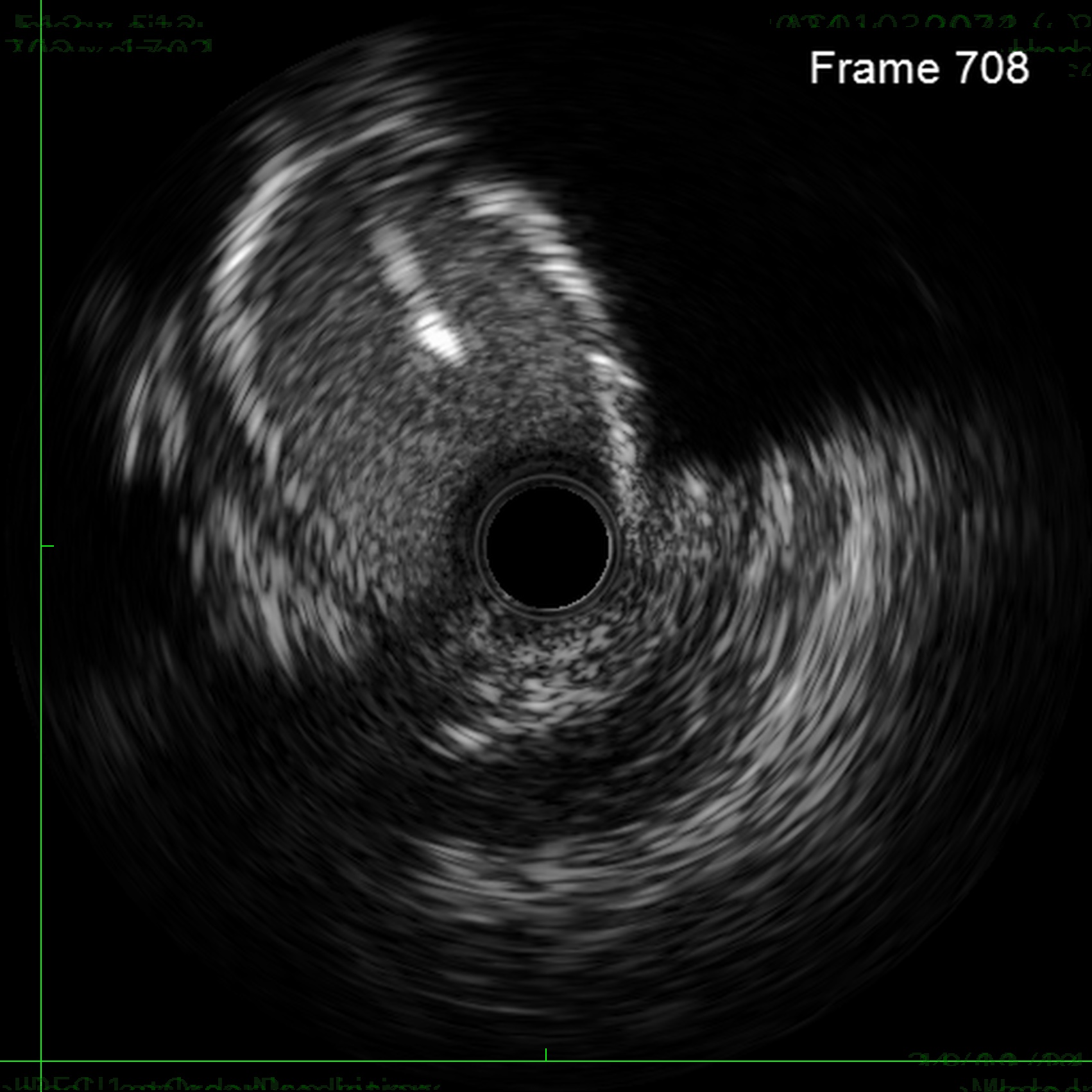
Procedural Step
Through bilateral femoral access, 7Fr EBU 3.5 and JR 4.0 catheters were engaged to the left main and RCA. With no antegrade entry, a retrograde marker wire and IVUS-guided antegrade puncture using Gaia Next 2 and Conquest Pro with Finecross failed, as both wires were deflected by the calcified cap despite tip modification with a secondary curve. A retrograde attempt using Gaia Next 2 and 3 with Finecross also failed.Suspecting LAD angulation, an antegrade re-attempt was performed using IVUS-guided puncture with a Conquest Pro 8-20 supported by a Supercross90 under retrograde wire guidance, successfully puncturing the proximal cap. Supercross was exchanged for Finecross, and the wire crossed distally, but Finecross and Corsair Pro XS could not advance due to the tight lesion. After proximal preparation and the anchor balloon technique in the LCx, the microcatheter advanced distally and the wire was exchanged for a workhorse wire. Retrograde injections confirmed true lumen position, and the LAD was predilated.
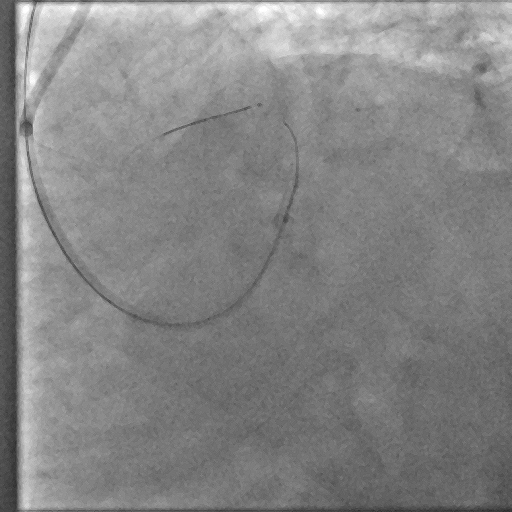
Antegrade Conquest pro 2nd curve IVUS guided puncture Unsuccessful.mp4
Antegrade Conquest pro 8-20 supercross IVUS guided puncture Spider.mp4
Antegrade Conquest pro 8-20 supercross IVUS guided puncture MC Tip Injection.mp4
Case Summary
This case demonstrates a complex left main bifurcation with a blunt ostial LAD CTO and tight ostial LCx stenosis, successfully managed through a hybrid strategy. When both antegrade and retrograde approaches failed, IVUS-guided puncture with a Supercross-supported high–tip-load wire enabled successful revascularization. The angulated microcatheter preserved the wire’s penetration force, allowing puncture of the proximal cap. Procedural safety was enhanced by a retrograde marker and tip injection confirming distal cap position, while intravascular imaging provided the precision required for safe execution and optimal procedural outcomes.