Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251021_001
One Mistake, Change My Life
By Saroj Hattakitpanitchakul
Presenter
Saroj Hattakitpanitchakul
Authors
Saroj Hattakitpanitchakul1
Affiliation
Chaophraya Yommaraj Hospital, Thailand1
View Study Report
CASE20251021_001
Coronary - Complex PCI - In-Stent Restenosis
One Mistake, Change My Life
Saroj Hattakitpanitchakul1
Chaophraya Yommaraj Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
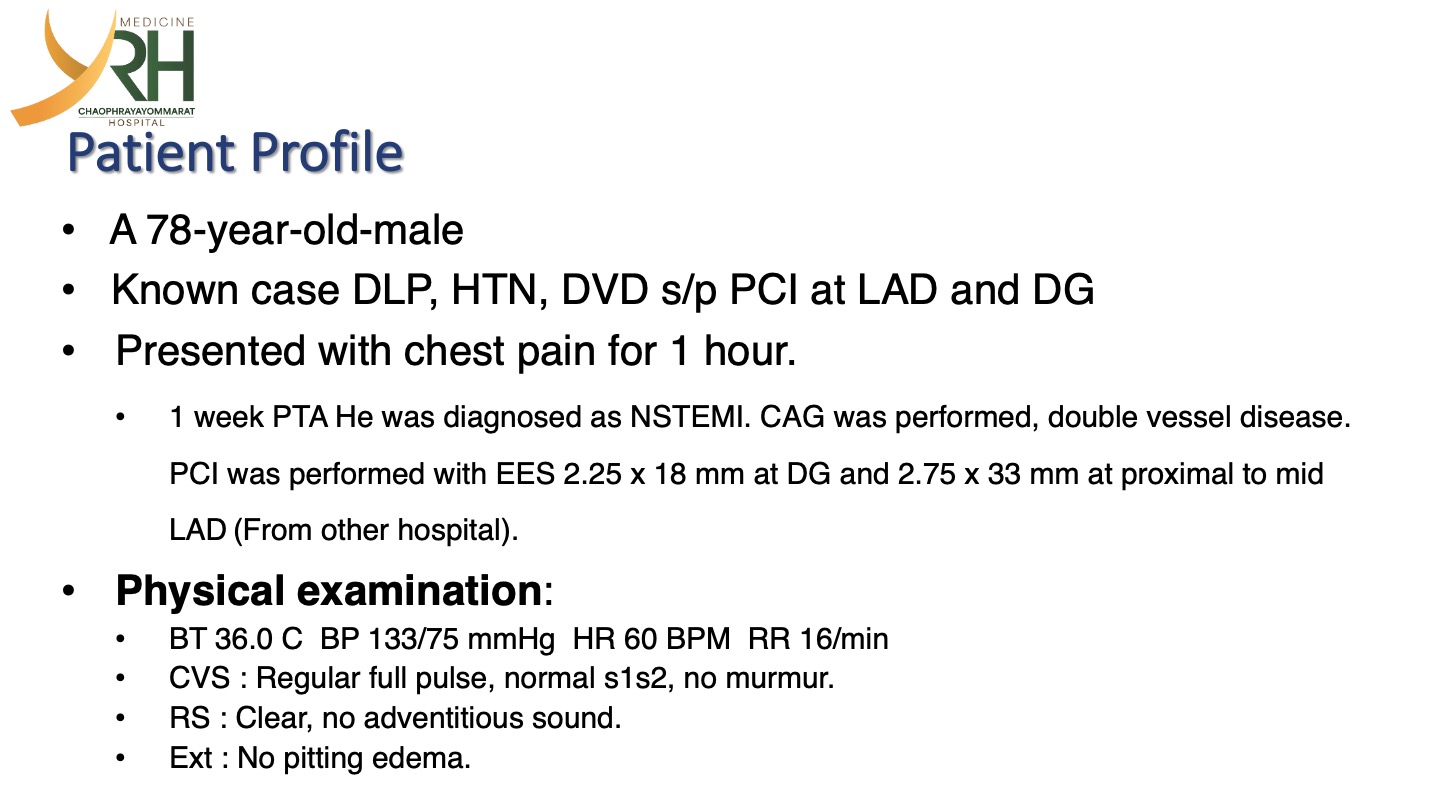
A 78-year-old-male Known case DLP, HTN, DVD s/p PCI at LAD and DGPresented with chest pain for 1 hour. • 1 week PTA He was diagnosed as NSTEMI. CAG was performed, double vessel disease. PCI was performed with EES 2.25 x 18 mm at DG and 2.75 x 33 mm at proximal to mid LAD (From other hospital).Physical examination:• BT 36.0 C BP 133/75 mmHg HR 60 BPM RR 16/min• CVS : Regular full pulse, normal s1s2, no murmur.• RS : Clear, no adventitious sound.• Ext : No pitting edema.
Relevant Test Results Prior to Catheterization
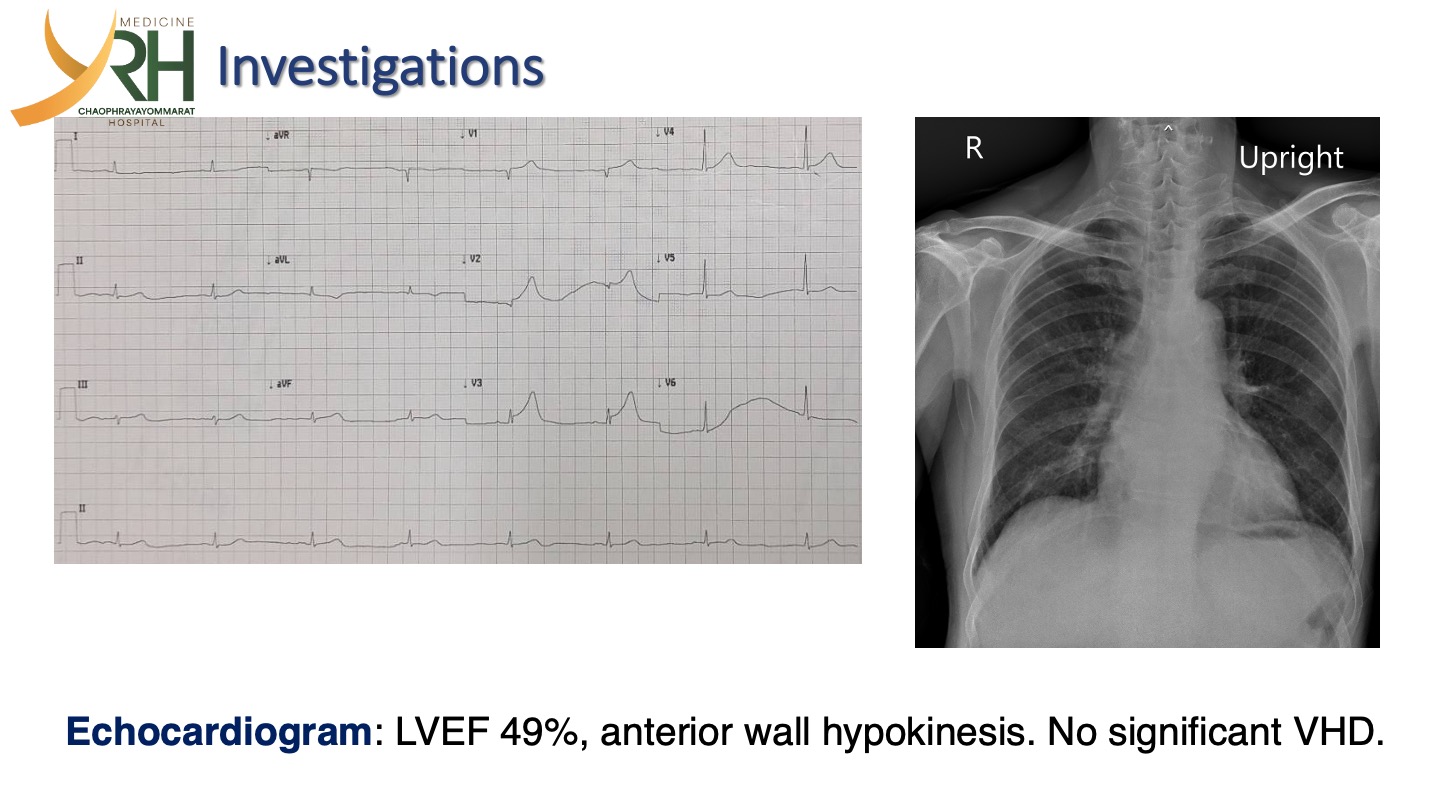
ECG sinus bradycardia with STE at V1-3.Echocardiogram: LVEF 49%, anterior wall hypokinesis. No significant VHD.CXR: Borderline cardiomegaly. No widening mediastinum.
Relevant Catheterization Findings
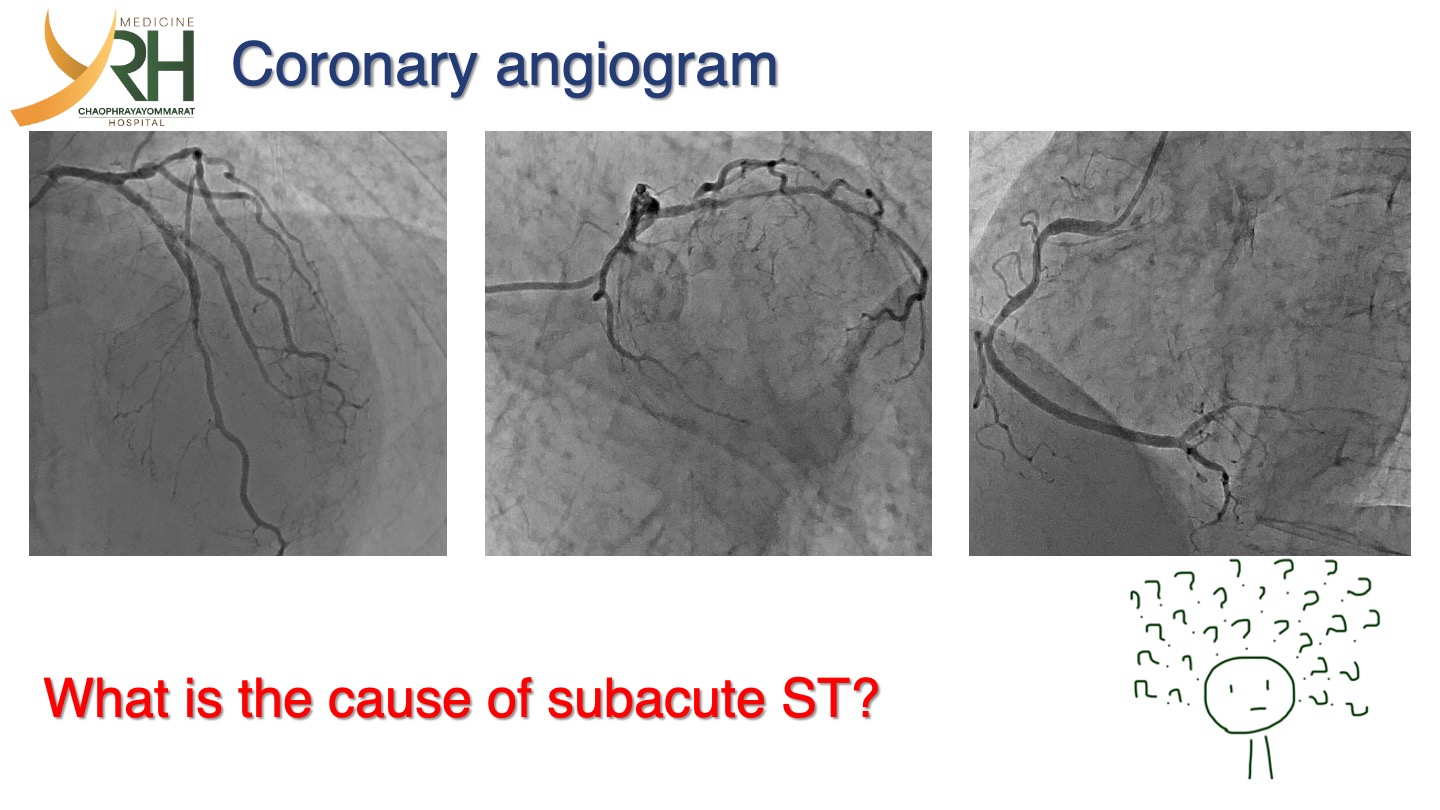
CAG: Luminal haziness and significant stenosis at proximal to mid LAD and DG stent. Significant stenosis at distal LCx.
 LCA R cra.mp4
LCA R cra.mp4
LCA L cau.mp4
Interventional Management
Procedural Step
First PCI
Final L cra.mp4
Final R cra.mp4
- Successful wiring with Sion GW to DG and Sion Blue GW to LAD.
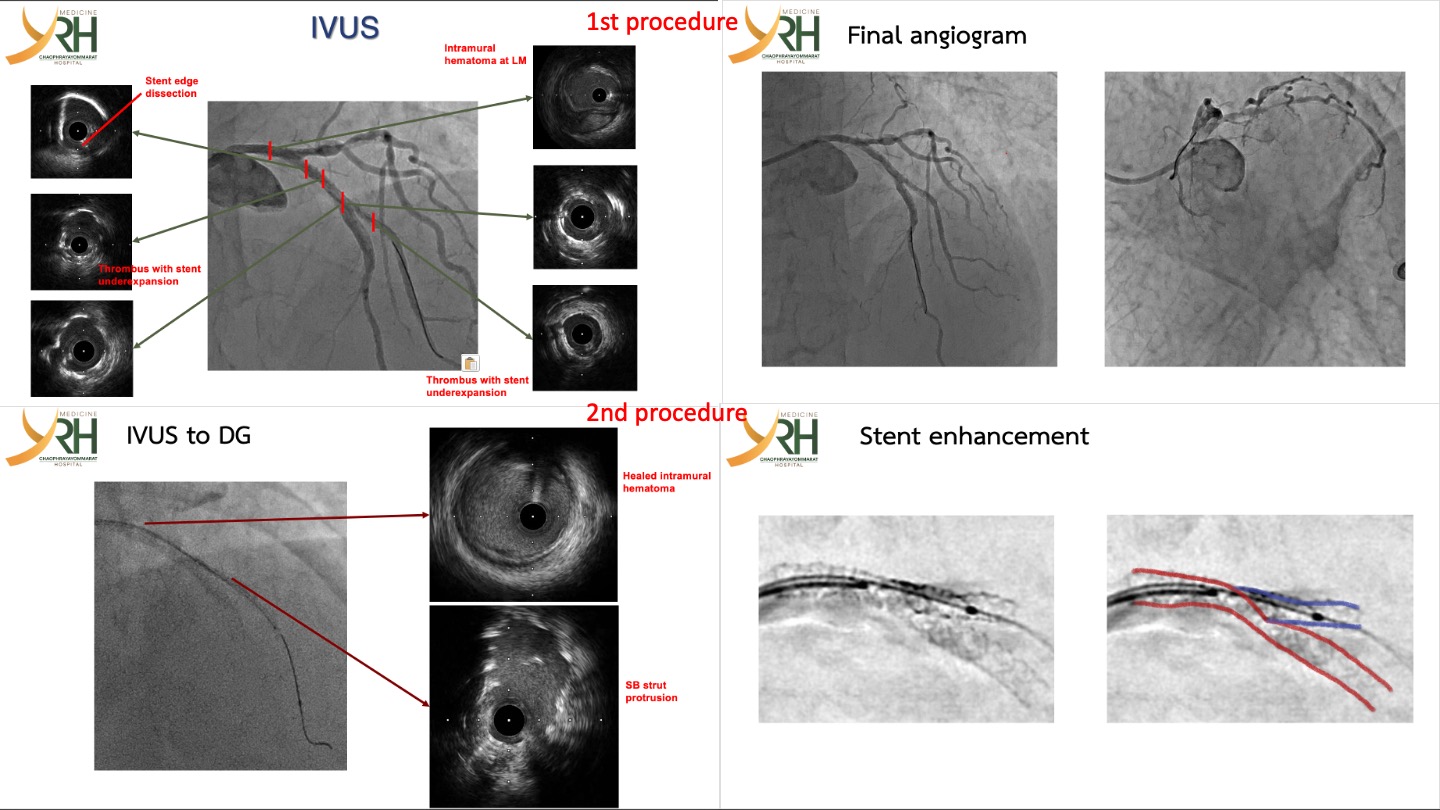
- IVUS was pulled back from DG and LAD
- Stent underexpansion with intraluminal thrombus at LAD and DG stent.
- Proximal edge of LAD stent dissection and intramural hematoma extending to LM.
- POBA with 3.0 x 15 mm NC balloon along LAD stent.
- POBA with 2.5 x 16 mm NC balloon along DG stent.
- After POBA at LAD/DG stent, 3.0 x 15 mm NC balloon, 1.5 x 15 mm SC balloon and IVUS could not cross to mid LAD.
- Final angiogram showed TIMI 3 flow and no residual significant stenosis. His chest pain was free.
- Successful wiring with Sion Blue GW to LAD.
- IVUS was inserted to LAD but could not crossed to mid LAD (Distal to LAD/DG bifurcation).
- Swap Sion Blue GW from LAD to DG.
- IVUS was pulled back from DG stent and showed stent strut protrusion to LAD.
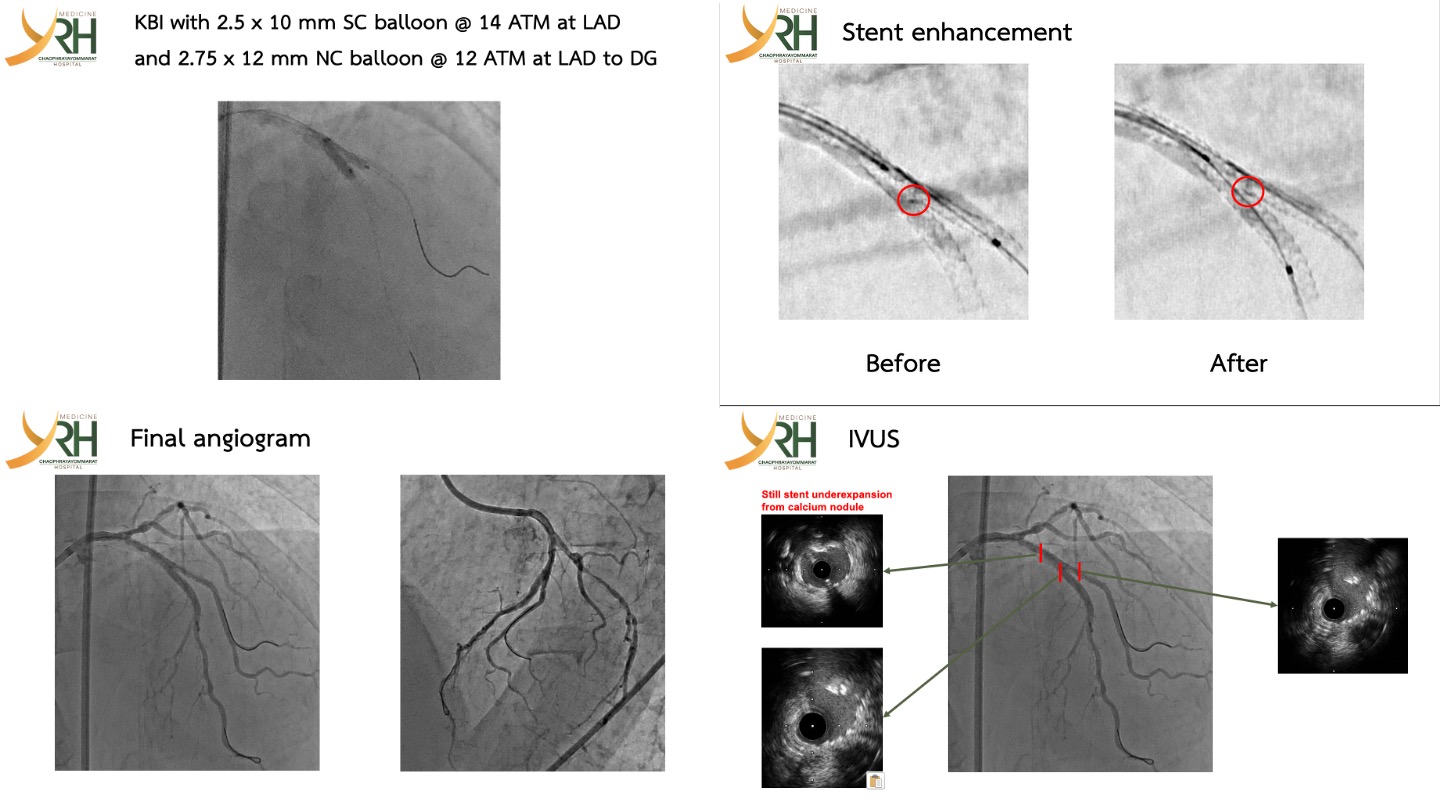
- Stent enhancement also showed the protruding strut at LAD/DG bifurcation as IVUS.
- Wiring with Sion GW to LAD.
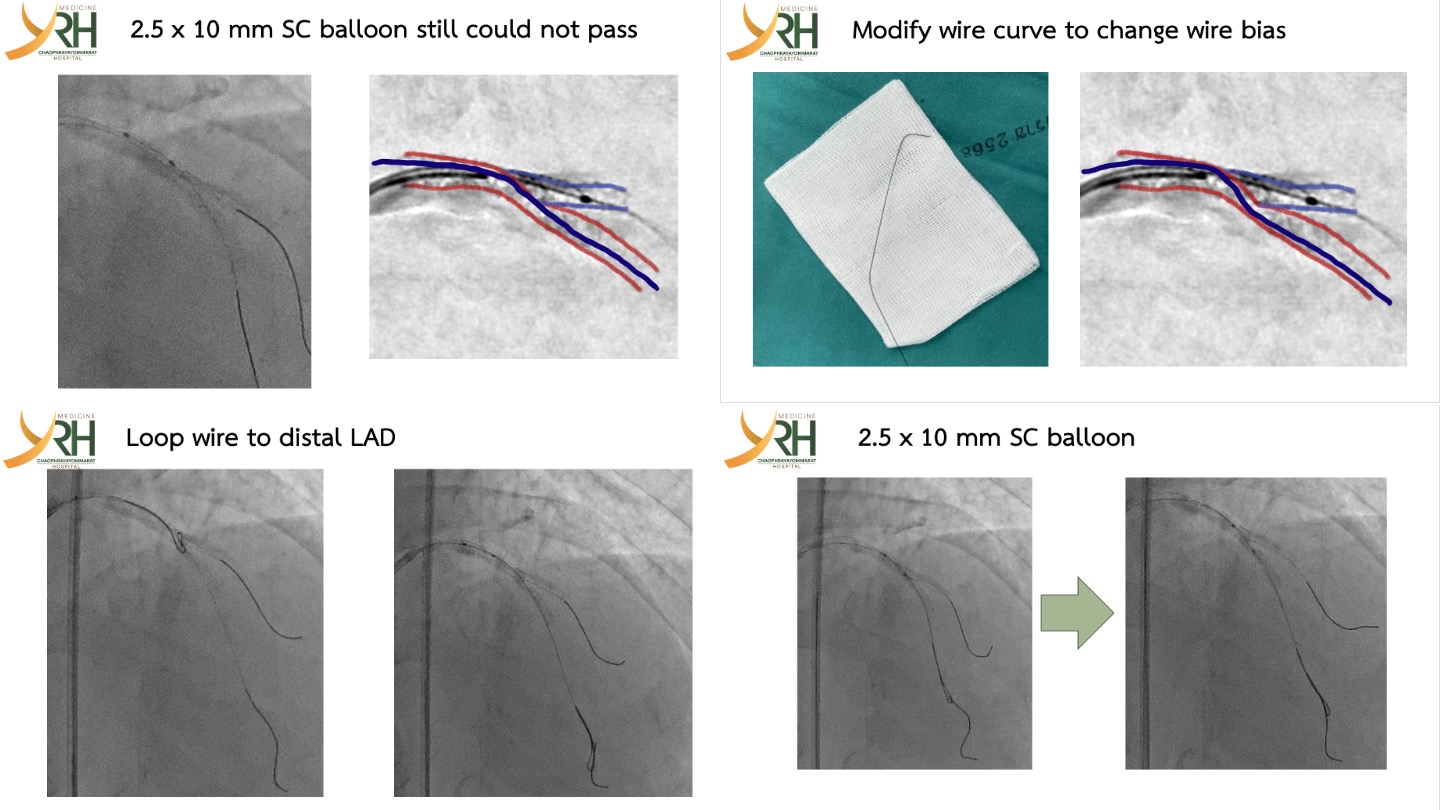
- 2.5 x 10 mm SC balloon could not cross to mid LAD.
- To overcome the crossing failure, we decided to modify the wire curve to change the wire bias as picture.
- Inserted Fielder FC GW to distal LAD (with loop wire at LAD/DG bifurcation: to avoid abluminal wiring).
- Successful crossing 2.5 x 10 mm SC balloon to mid LAD.
- KBI with 2.5 x 10 mm SC balloon @ 14 ATM at LAD and 2.75 x 12 mm NC balloon @ 12 ATM at DG.
- IVUS was pulled back from LAD and DG and demonstrated as picture.
Case Summary
- The main branch balloon should be positioned at the bifurcation before side branch (SB) stent dilation to maintain access and facilitate final optimization.
- Intravascular imaging is essential to identify the cause of stent problem, uncrossable equipment and guide proper correction.
- When a balloon cannot cross after bifurcation stenting, possible causes include:
- - Abluminal wiring
- - Stent deformation
- - Wire bias
- Wire bias is a crucial factor affecting the ability to deliver equipment and achieve optimal stent expansion.