Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251019_002
The Second Strike: Retrograde Triumph in a Bifurcation Chronic Total Occlusion
By Cze Ci Chan, Ying-Chang Tung
Presenter
Cze Ci Chan
Authors
Cze Ci Chan1, Ying-Chang Tung1
Affiliation
Linkou Chang Gung Memorial Hospital, Taiwan1
View Study Report
CASE20251019_002
Coronary - Complex PCI - CTO
The Second Strike: Retrograde Triumph in a Bifurcation Chronic Total Occlusion
Cze Ci Chan1, Ying-Chang Tung1
Linkou Chang Gung Memorial Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 65-year-old male with hypertension, dyslipidemia, and a history of smoking. He initially presented with an inferior wall ST-elevation myocardial infarction and underwent PCI with stenting to the distal RCA. He was readmitted three weeks later with unstable angina and received proximal RCA stenting, with a failed attempt to recanalize a CTO of the LCX. On examination, he is alert, hemodynamically stable, with clear lung fields, normal heart sounds, and no peripheral edema.
 1.AVI
1.AVI
2.mp4
3.AVI
Relevant Test Results Prior to Catheterization
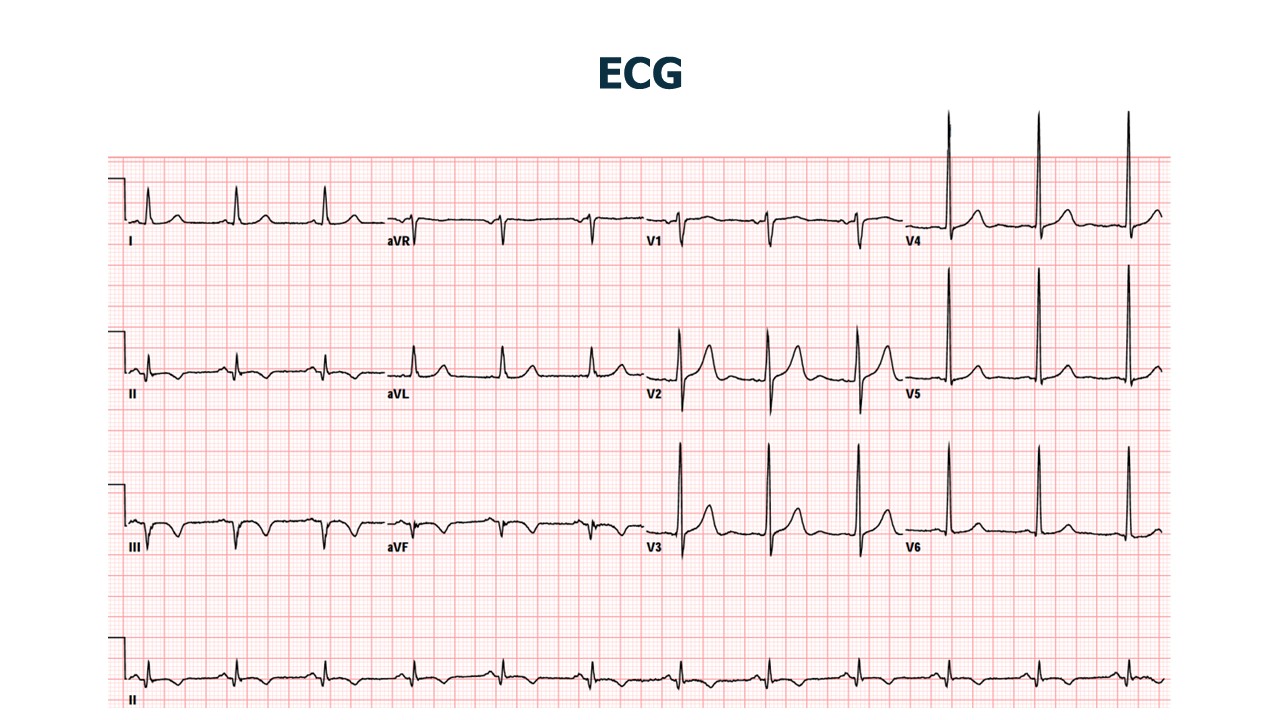
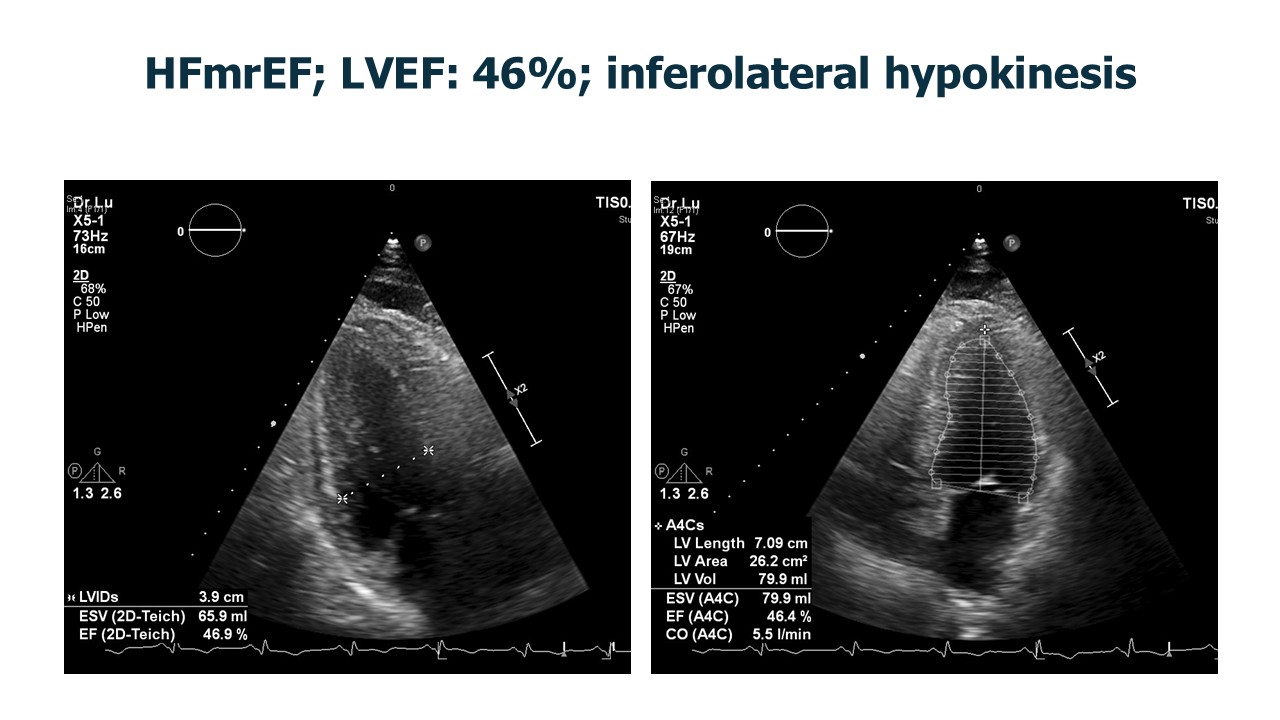
Complete blood count and renal function tests were within normal limits. Glycated hemoglobin was 5.7%. Lipid profile showed total cholesterol 157 mg/dL and low-density lipoprotein 99 mg/dL. B-type natriuretic peptide was elevated at 545 pg/mL. ECG demonstrated T-wave inversion over inferior leads, and echocardiogram revealed mildly reduced ejection fraction of 46% with inferolateral wall hypokinesis.
Relevant Catheterization Findings
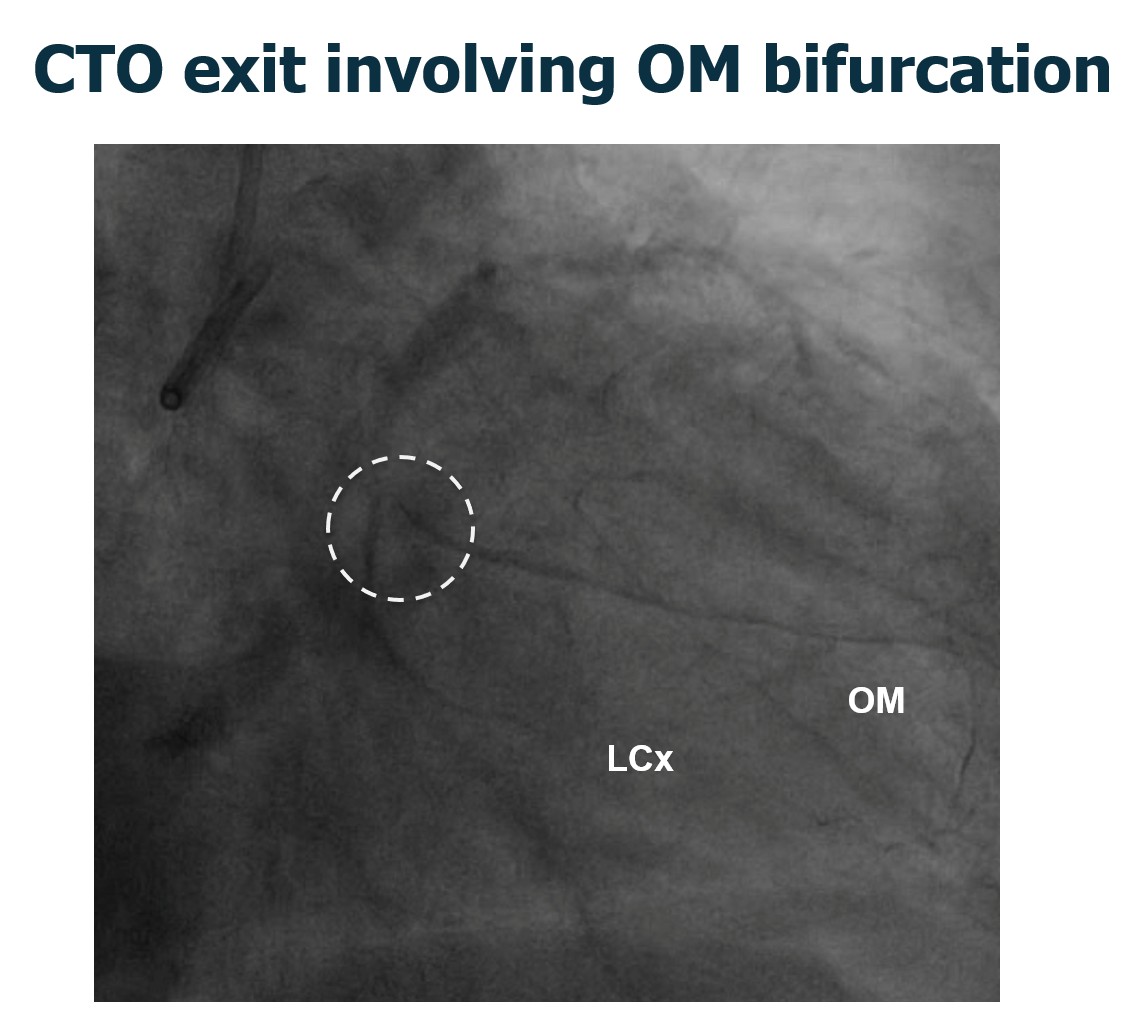
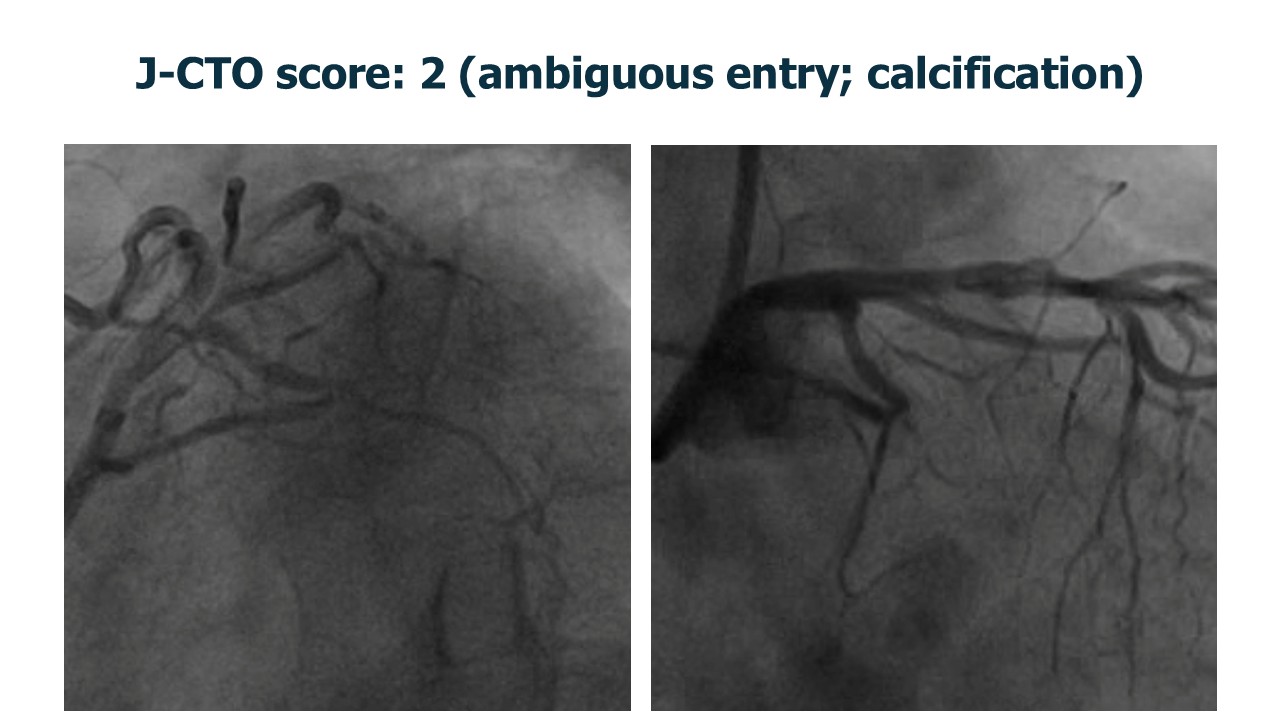
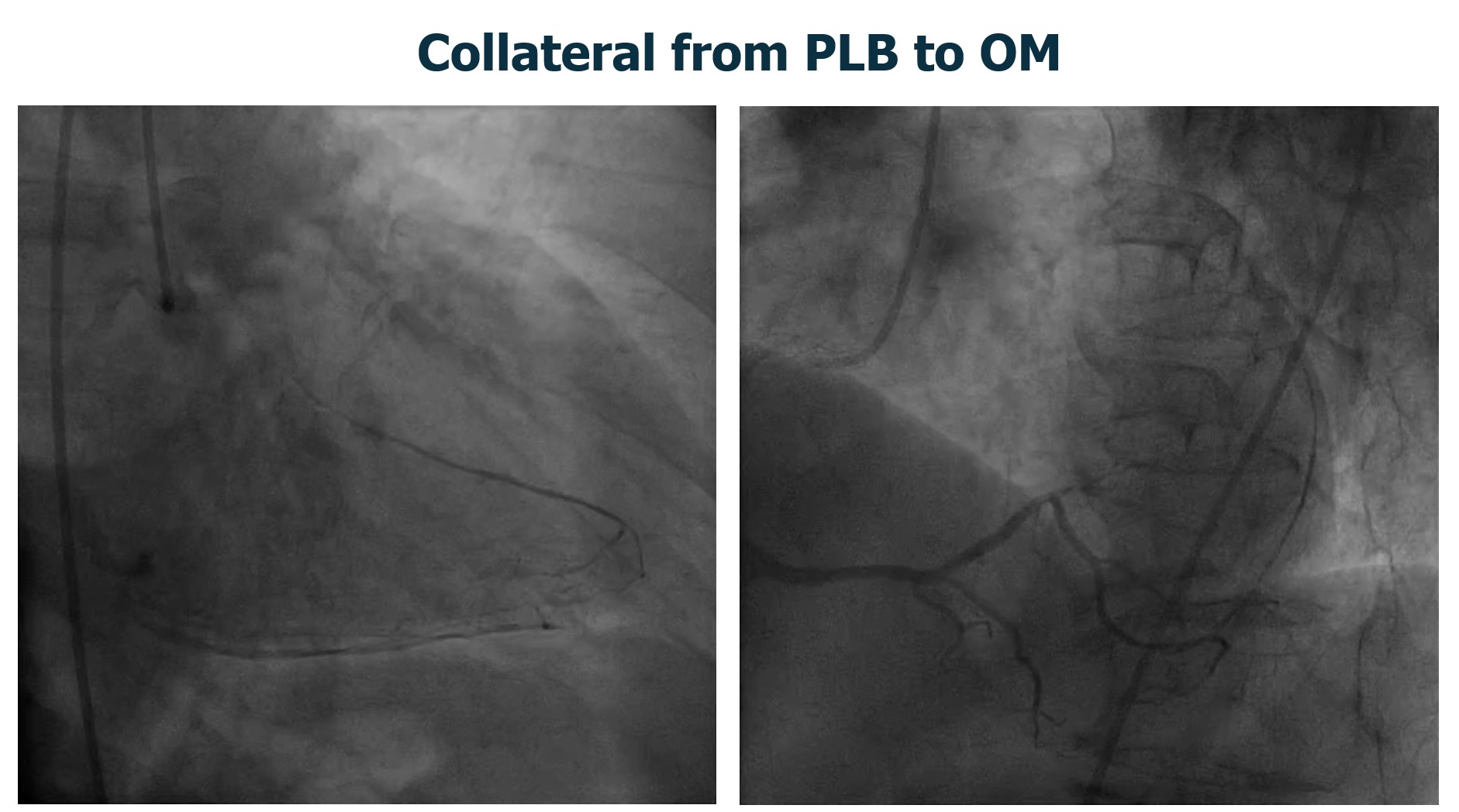
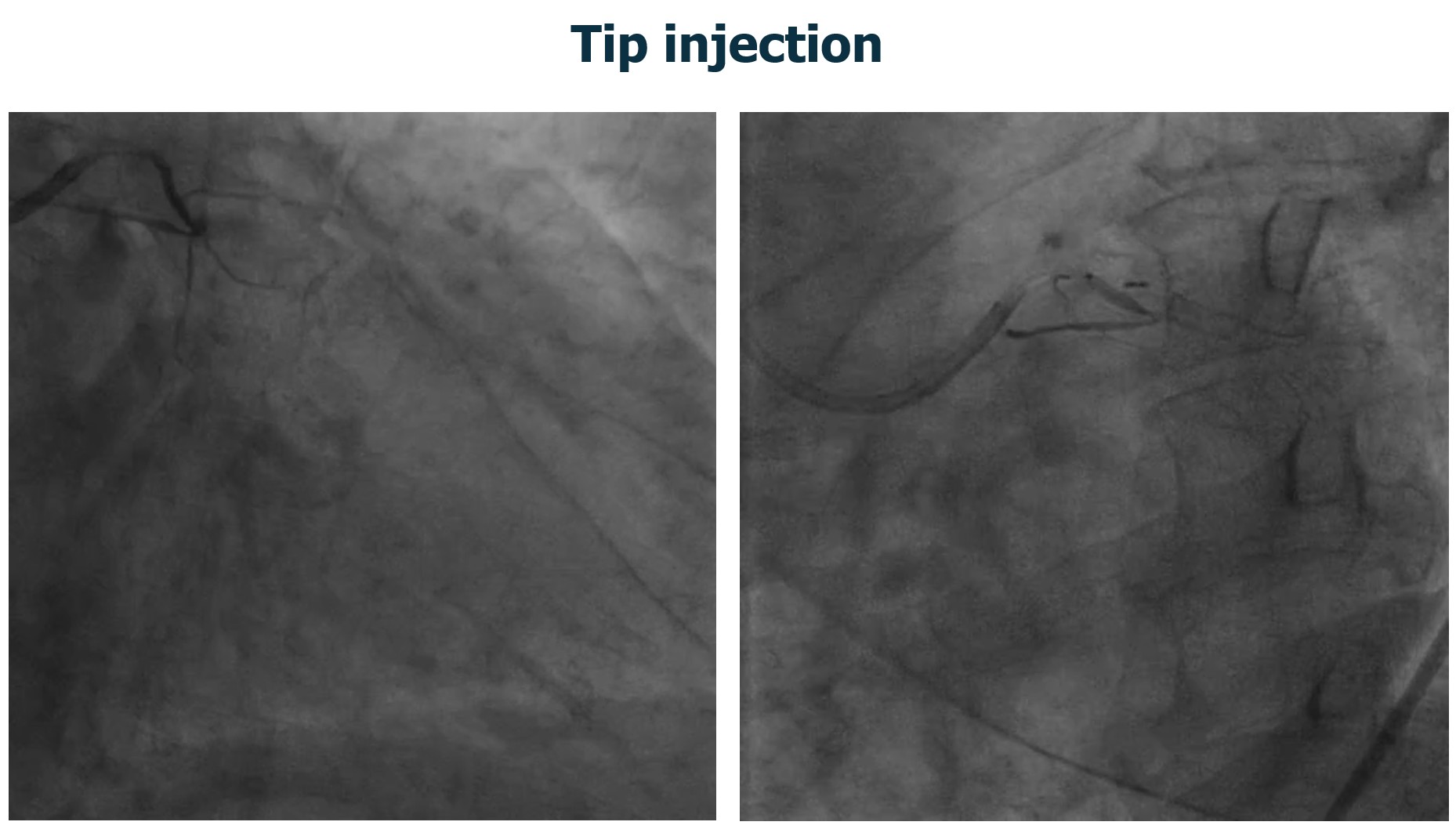
Coronary angiography demonstrated patent prior RCA stents. The LCX CTO had a J-CTO score of 3 (ambiguous proximal cap, calcification, and prior failed attempt). Distal LCX was opacified via epicardial collaterals from the PL branch. Antegrade tip injection failed to reveal bridging collaterals or a definable micro-channel for entry, making antegrade crossing unfavorable.
3-1.mp4
3-2.mp4
Interventional Management
Procedural Step
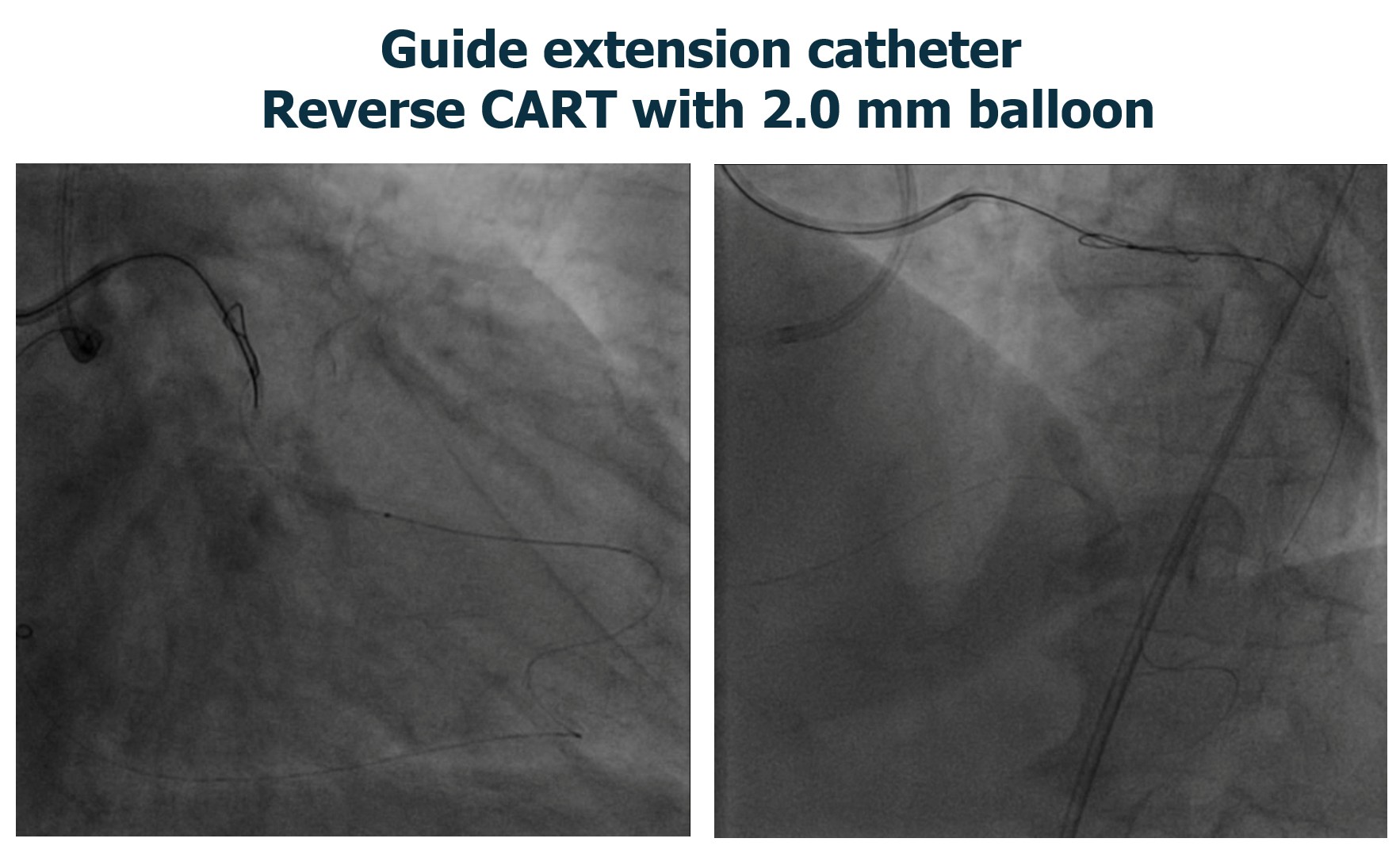
Bilateral coronary engagement with double guiding catheters was used to support both antegrade and retrograde strategies. A retrograde approach through the PL branch was performed, with a microcatheter advanced through epicardial collaterals to the distal OM. Reverse CART was done to create a connection between the antegrade and retrograde spaces.
A guide extension catheter–assisted tip-in technique was used to improve alignment and help convergence. The retrograde wire was then advanced into the antegrade microcatheter within the antegrade guide catheter. The antegrade microcatheter eventually advanced across the CTO over the retrograde wire to secure antegrade access for devices.
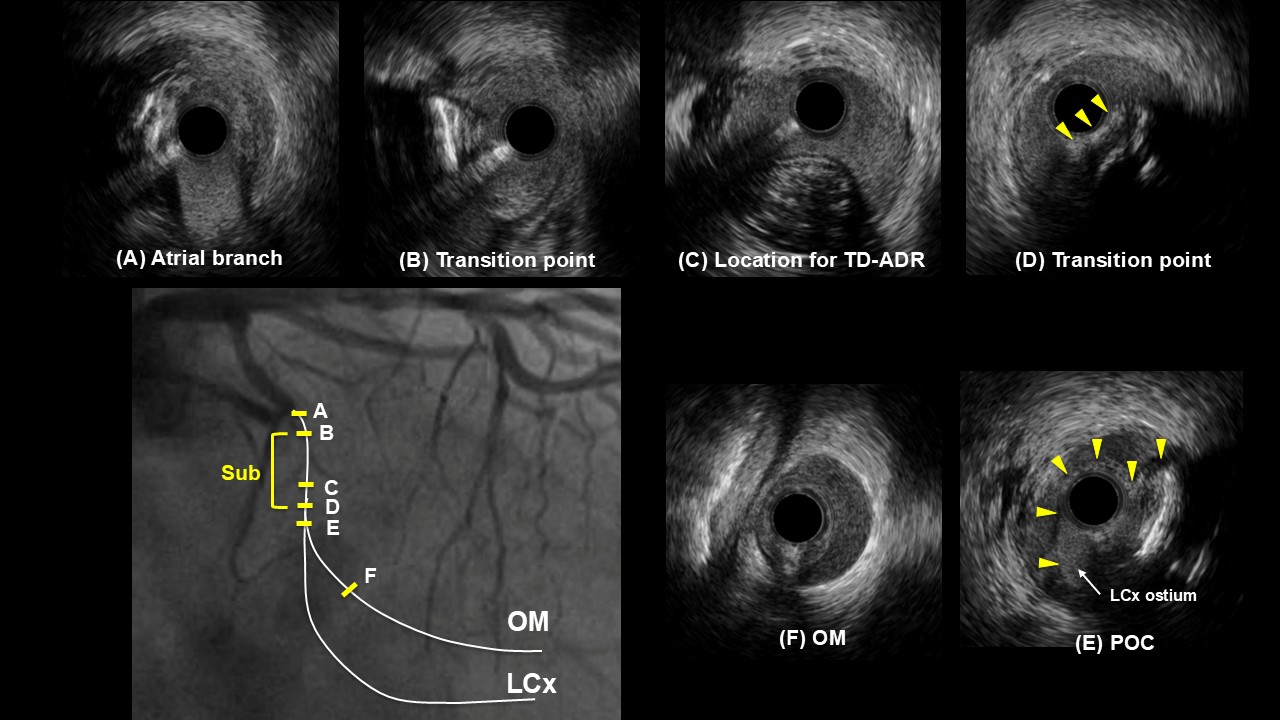
IVUS pullback from the OM showed a short segment of subintimal tracking before the LCX–OM bifurcation and a large hematoma from the bifurcation extending into the distal OM. Further wiring toward the distal LCX was attempted, and IVUS confirmed that the wire was located in the false lumen. The IVUS catheter was left in place within the false lumen to serve as a landmark. A second guiding catheter was then positioned, and using real-time IVUS guidance, a new wire was advanced from the second guiding catheter into the true LCX lumen across the bifurcation.
After true lumen access was achieved, provisional LCX to OM stenting restored TIMI 3 flow. Final IVUS showed good stent expansion and apposition, without edge dissection or residual hematoma.
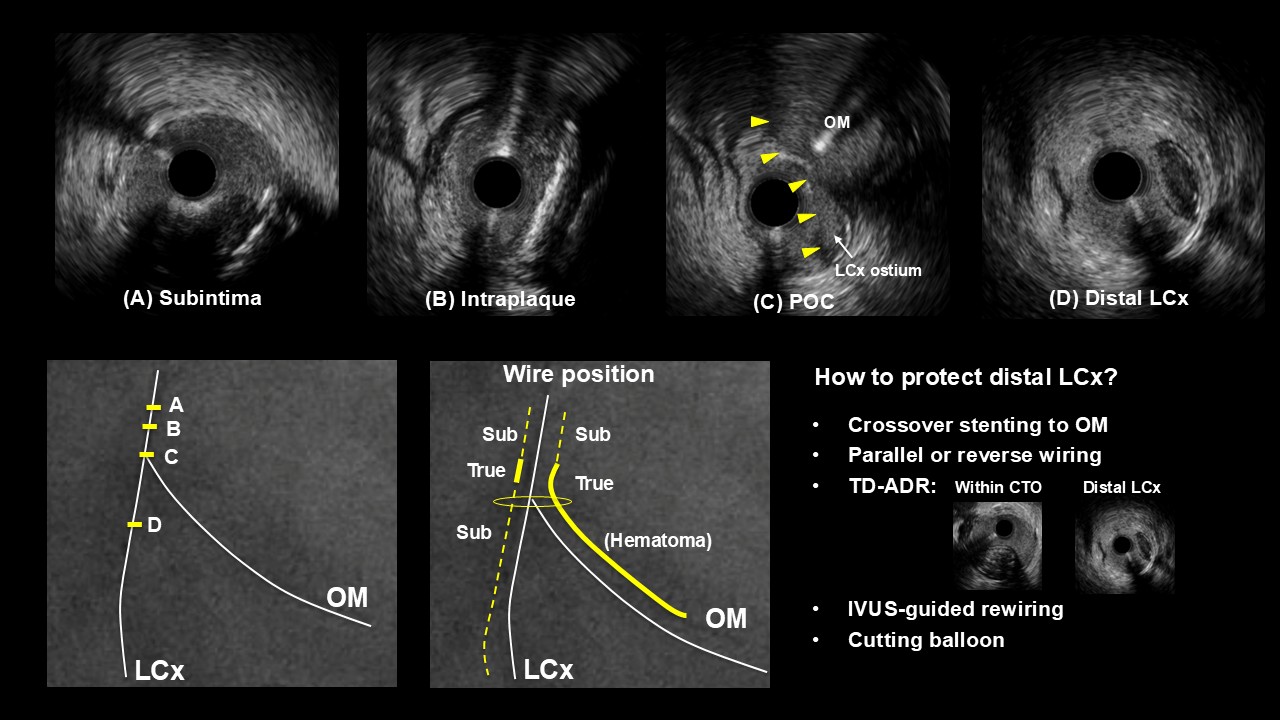
Case Summary
This case illustrates the value of a bidirectional strategy for complex distal bifurcation CTOs, where preservation of important side branches such as the OM is critical. The combination of retrograde techniques, guide extension catheter–assisted tip-in, and a double guiding catheter setup enabled controlled crossing and support. IVUS was essential at multiple stages to confirm wire position, detect subintimal passage and hematoma, and guide rewiring into the true lumen across the bifurcation.