Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251018_002
A Challenged Decision-Making for TAVR in Pre-Existing Effected Condition With High Complication Risk
By Apichat Jansillapakorn, Anuruck Jeamanukoolkit, Wasant Soonfuang, Sukhum Tachasakunjaroen, Sakolwat Montrivade
Presenter
Apichat Jansillapakorn
Authors
Apichat Jansillapakorn1, Anuruck Jeamanukoolkit1, Wasant Soonfuang1, Sukhum Tachasakunjaroen1, Sakolwat Montrivade1
Affiliation
Police General Hospital, Thailand1
View Study Report
CASE20251018_002
Structural - Aortic Valve Intervention - Complex TAVR
A Challenged Decision-Making for TAVR in Pre-Existing Effected Condition With High Complication Risk
Apichat Jansillapakorn1, Anuruck Jeamanukoolkit1, Wasant Soonfuang1, Sukhum Tachasakunjaroen1, Sakolwat Montrivade1
Police General Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
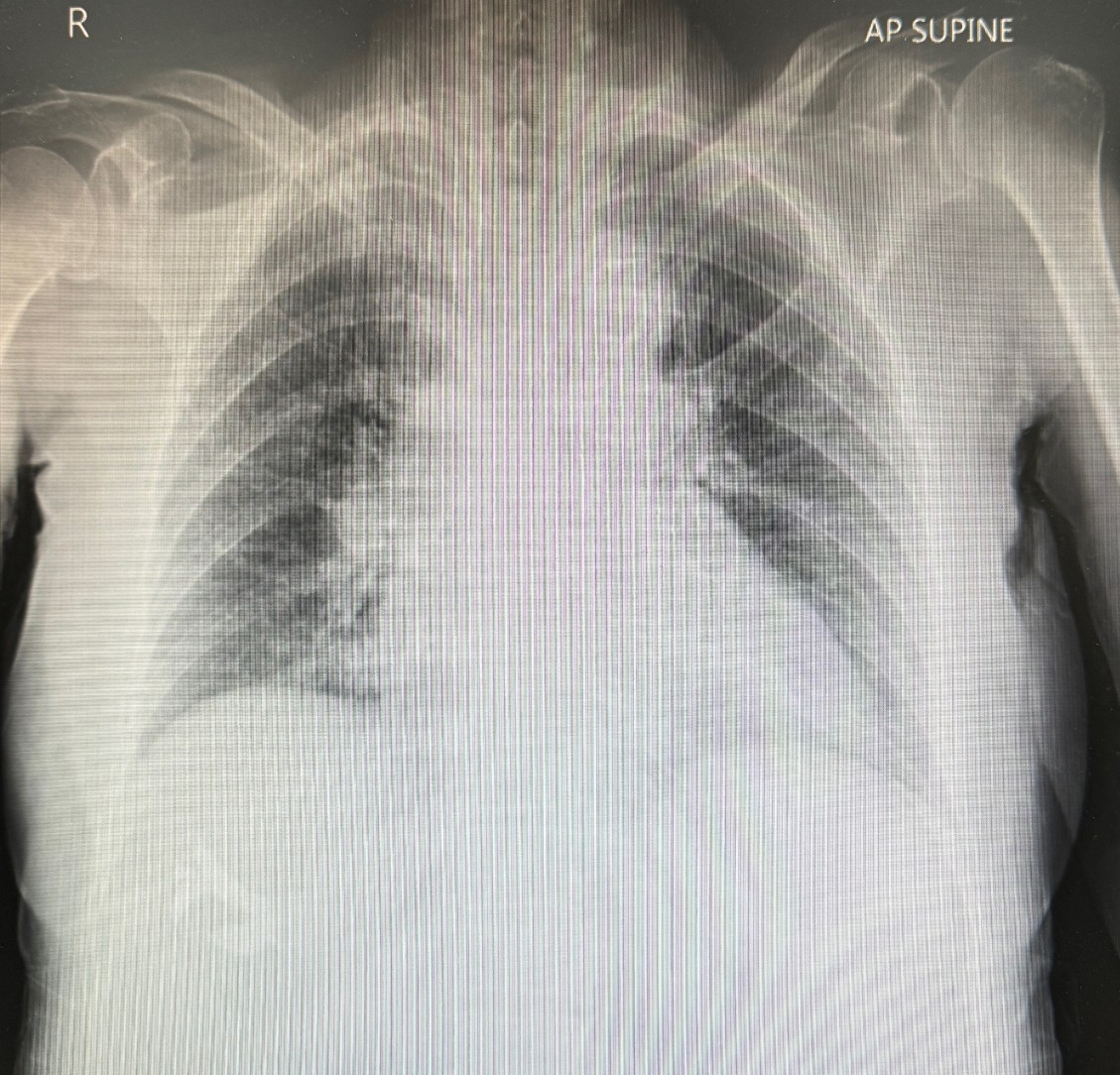
A Thai 97-year-old woman, who's totally independent, documented history of AF with severe TR S/P T-TEER for 4 years ago, HTN, DLP, mild dementia. She presented with a 12-month history of unspecified exertional dyspnea, NYHA III. Physical examination revealed stable hemodynamics, well-orientation with sign of chronic heart failure and LVH. Appearing peripheral abnormalities on palpation and murmur on auscultation, which's compatible with severe tricuspid regurgitation and severe aortic stenosis.
 TCTAP2026-PreTAVR ECHO.mp4
TCTAP2026-PreTAVR ECHO.mp4
Relevant Test Results Prior to Catheterization
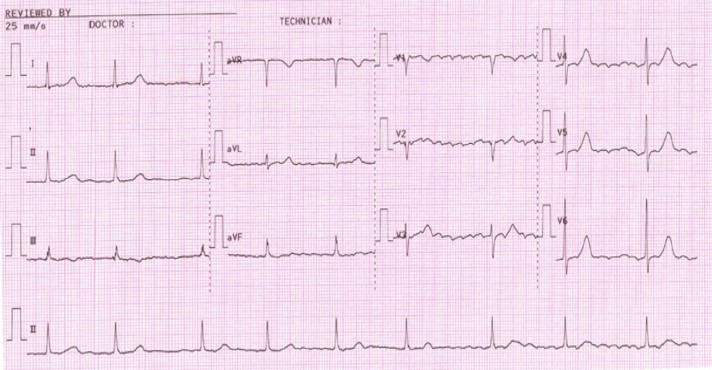
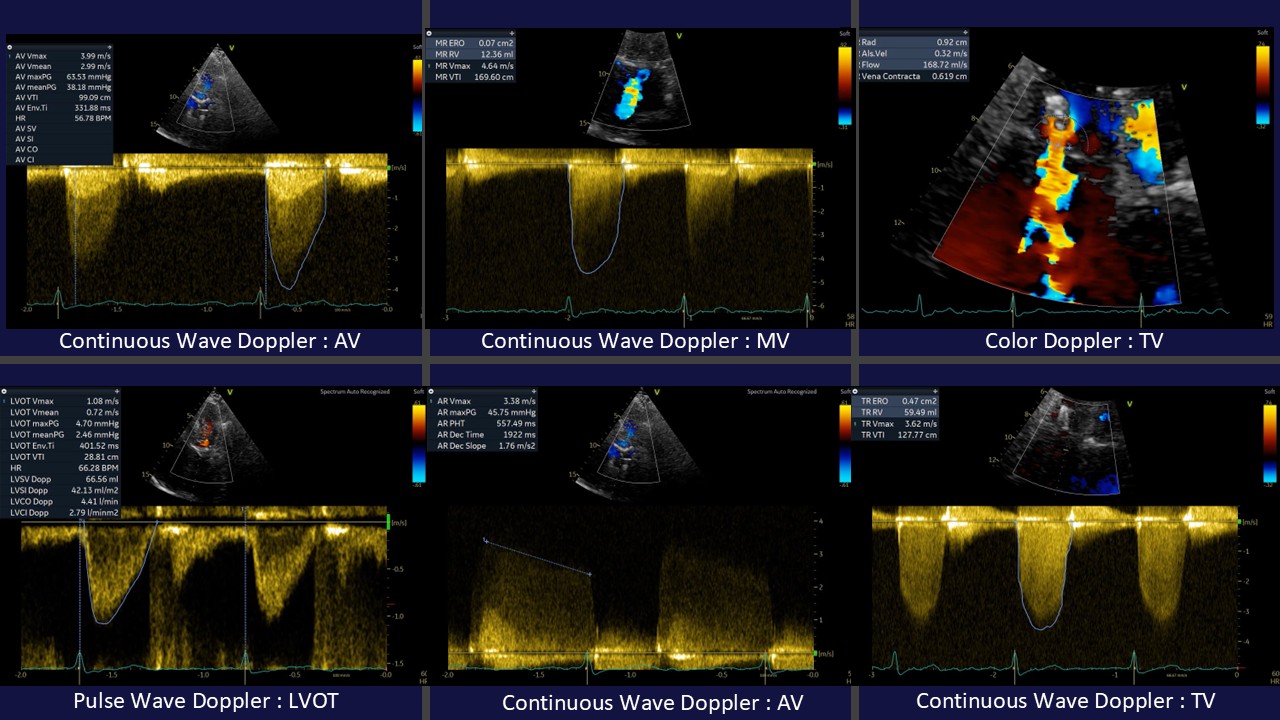
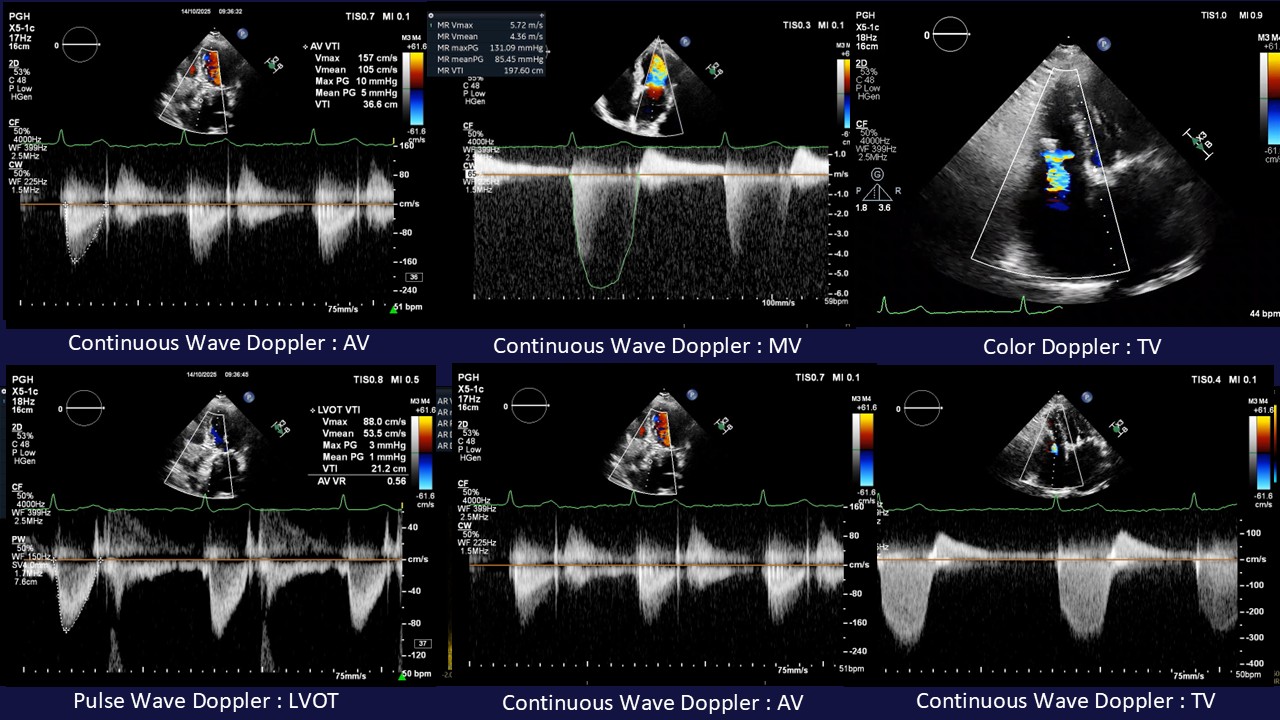
Her ECG revealed AF without pre-existing BBB. Transthoracic echocardiography revealed concentric LVH with 65% of LVEF, severe biatrials enlargement, normal RV function , multiple heart valve abnormalities indicated to a TriClip device with severe TR, moderate functional MR and severe calcific aortic stenosis. As the Heart Team discussion, several cause of symptoms was suspected. We brain stormed to design her individual appropriated-solution, on concerning of natural history in each disease.
TCTAP2026-TAVR CAG.mp4
Relevant Catheterization Findings
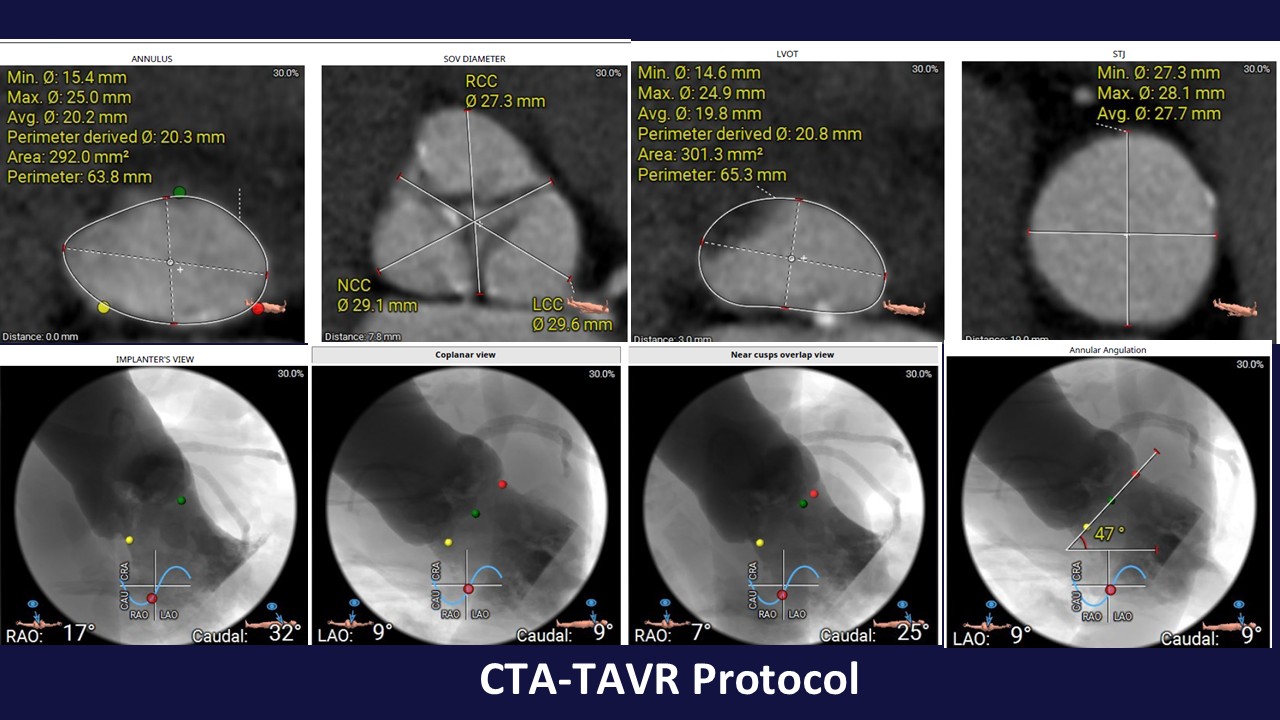
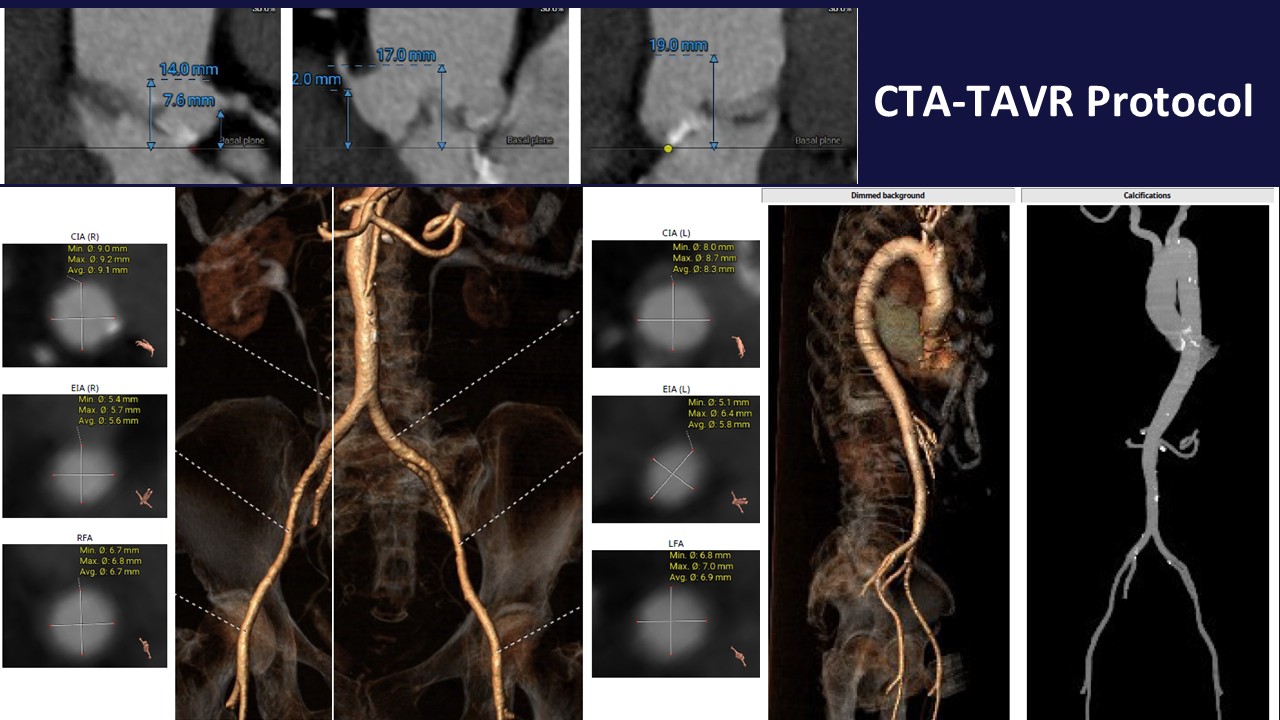
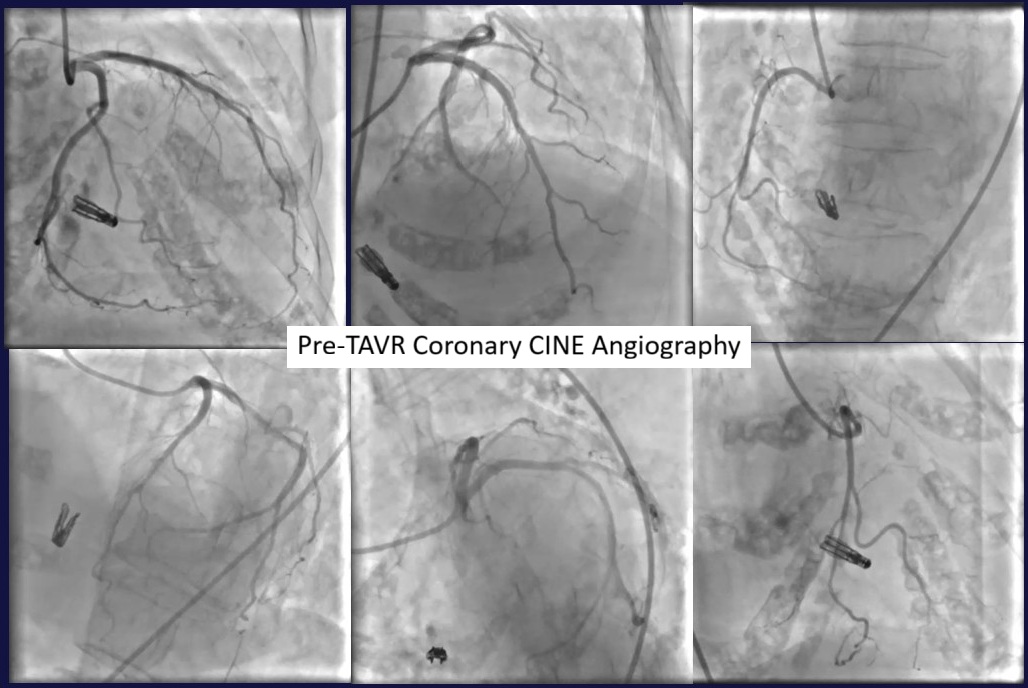
The patient was performed multimodality of investigations in many medical center, evaluating symptoms. The first, CAG showed non-obstructive CAD. CTA as TAVR protocol identified challenge issue of low LCA ostial (7.6 cm.), low aortic valve calcium, addition to concerning of a-step for pacing control across TriClip. We decide to perform TAVR first, followed by re-evaluating MR and TR. Because intervalvular disturbance may occur in multivalvular heart disease, leading valves' severity misestimation.
TCTAP2026 - TAVR Procedure.mp4
Interventional Management
Procedural Step
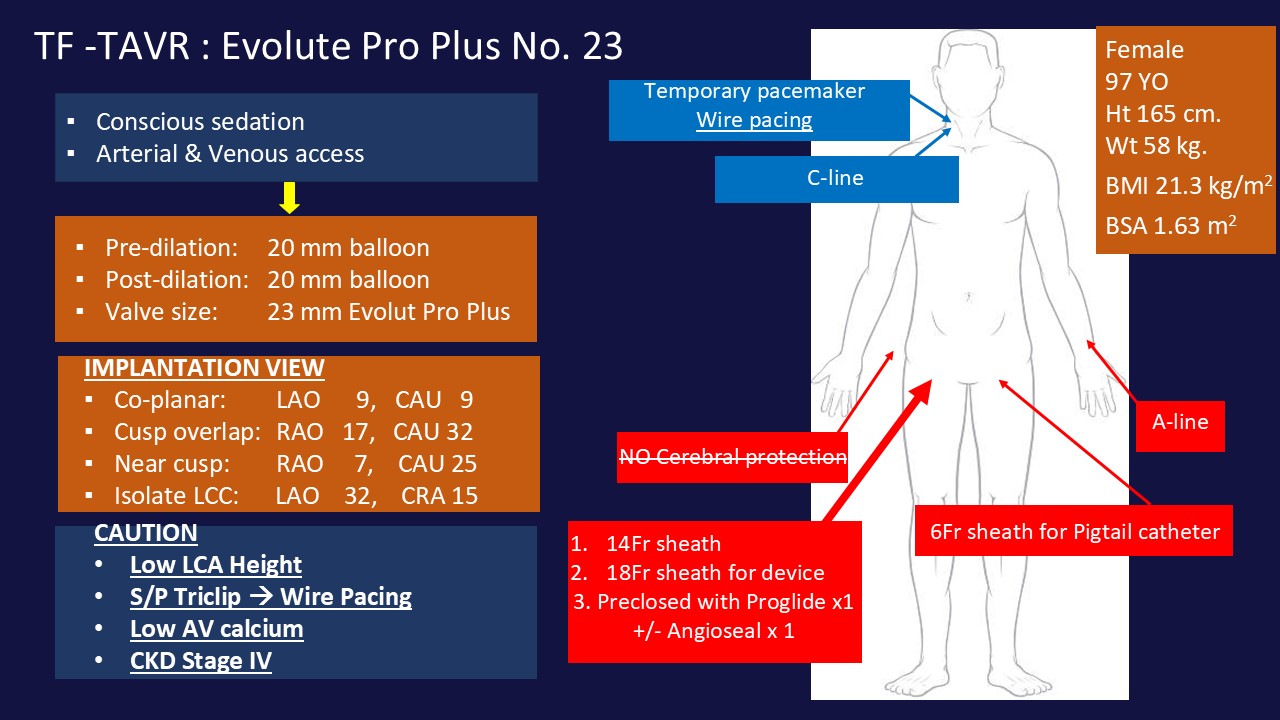
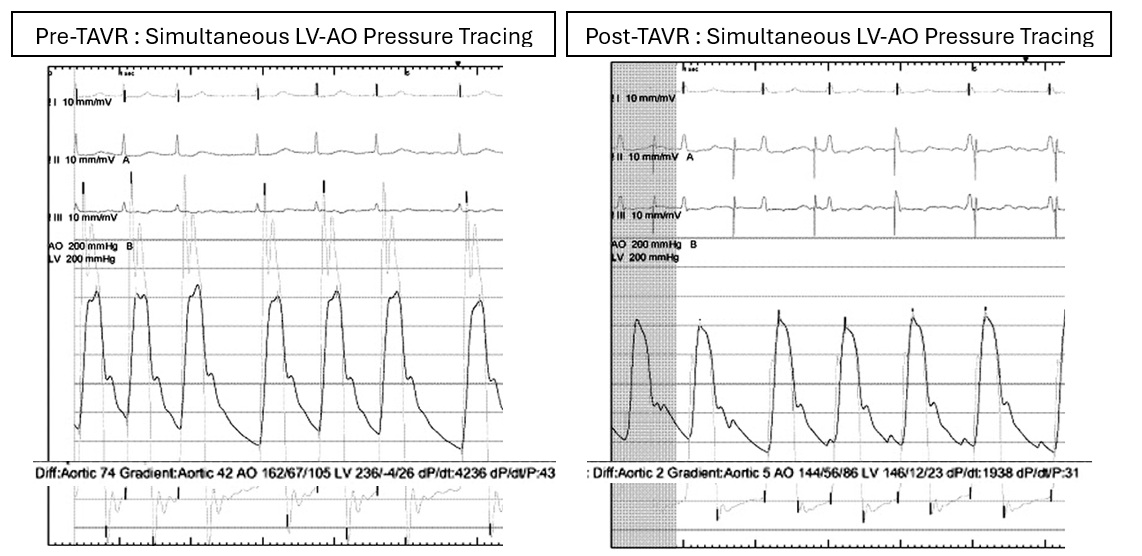
Conscious sedation was performed and common femoral artery with 14Fr long sheath was applied. long According to complication concern, we perform FA-TAVR with self-expandable-supra annular THV which'd proper waist for her LCA ostial. After LV-AO gradient assessment of 42 mmHg, we decided to pre-dilated by 20x40 mm. VAC III balloon over 0.035Confida wire. Because of pre-existing TriClip, LV wire pacing was utilized in this case. Self-expandable with supra-annular THV was designed for LCA obstruction, the THV waist and SOV diameter were evaluated appropriately along with LCA height, and Cusp over view (RAO17, CAU32) for avoid BBB was used. Although her had low AV calcium, but small LVOT was not be additional risk factor for THV embolization because. Improvement of LV-AO pressure gradient reduction to 4-5 mmHg., trivial paravalvular leak, significant MR and TR reduction were detected after finished procedure. Application of 2 Proglide vascular closure devices assisted puncture site complication was disappear. The patient went out from hospital in next 72hr. later, clinical NYHA II without early complication, transthoracic echocardiography revealed appreciated result for THV implantation. Further that, significant reduction of MR and TR were good predictor for overall long term result. However, concerned-valvular condition had remained in chart, especially progression of secondary MR from atrial fibrillation that might be adjusted by another TEER. Life-long DOACs also be applied.
TCTAP2026-PostTAVR ECHO.mp4
Case Summary
Among TAVR ERA belong with aging society, concerned condition for TAVR was discovered more and more, and inevitable. Heart team's procedural planning had still be necessary step to achieved the most suitable THV, smooth procedural period and appreciated clinical out come. Something out of guideline could find a way out by pathophysiology or step-by-step solution. Challenged in multivalvular condition, the investigation could reveal severity under-or overestimation that mislead treatment, repeated-assessment needed.