Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251014_001
A Rare Case of PCI in a Single Coronary Artery Arising as a Common Trunk From Right Coronary Sinus Presenting With Acute Myocardial Infarction
By Vipin Thomachan, Akash Vipin Thomas
Presenter
Vipin Thomachan
Authors
Vipin Thomachan1, Akash Vipin Thomas2
Affiliation
STMC, United Arab Emirates1, Amrita Institute of Medical Sciences, India2
View Study Report
CASE20251014_001
Coronary - ACS/AMI
A Rare Case of PCI in a Single Coronary Artery Arising as a Common Trunk From Right Coronary Sinus Presenting With Acute Myocardial Infarction
Vipin Thomachan1, Akash Vipin Thomas2
STMC, United Arab Emirates1, Amrita Institute of Medical Sciences, India2
Clinical Information
Relevant Clinical History and Physical Exam
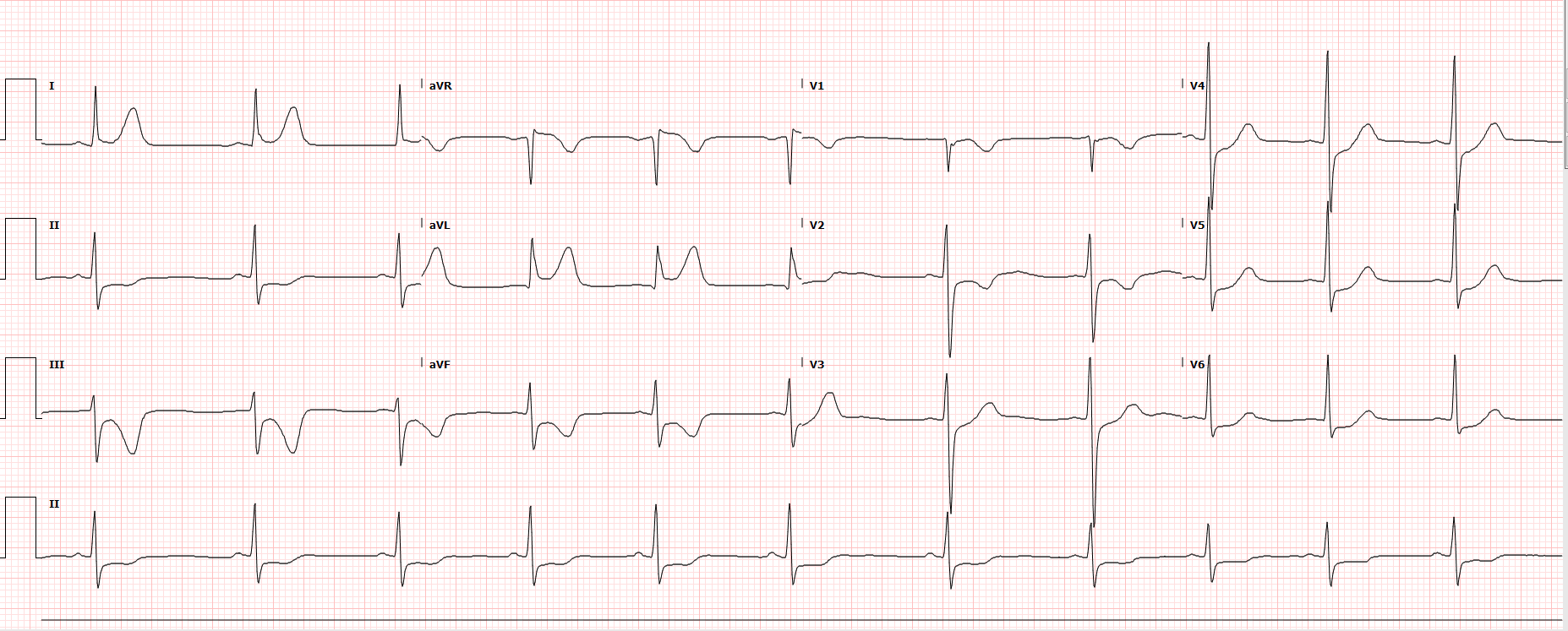
A 35yr old male patient with strong family history of coronary artery disease presented with non-ST elevation myocardial infarction (NSTEMI). He did not have any other known conventional risk factors or co-morbidities. ECG showed inferior ST depression and transient subtle ST elevation in I & aVL.
Relevant Test Results Prior to Catheterization
Cardiac Troponin T elevated at 267ng/LCreatinine 71 micro mol/LeGFR 127 ml/minHb 15.4g/dLHb A1c 6.4%
Relevant Catheterization Findings
Coronary angiography was performed through right radial approach using 5F TIG catheter. Left coronary sinus contrast injection failed to show any coronary artery origin despite multiple attempts. Right coronary sinus injection showed a coronary artery arising from right coronary cusp as a single trunk which divides into RCA and left system. Left system further divides into LAD and LCX. Mid RCA showed a very tight concentric severe stenosis. Left system was devoid of any significant disease.

Interventional Management
Procedural Step
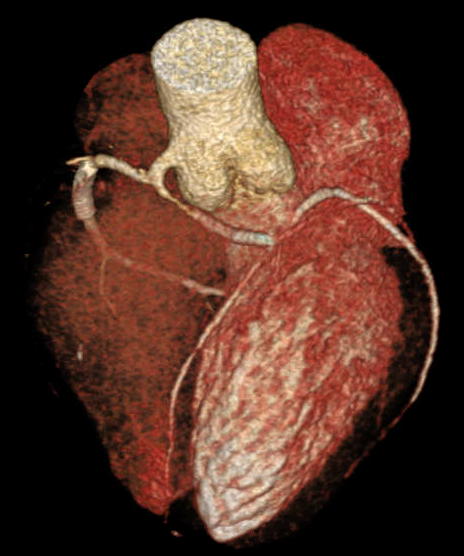
Percutaneous Coronary Intervention (PCI) of mid RCA: Common coronary trunk ostium was engaged with a 6F JR4.0 guiding catheter with meticulous care to prevent any ostial injury. Mid RCA lesion crossed with a 0.014” BMW wire. Predilated the lesion with 2.5x12mm semi compliant balloon. Stenting of the lesion was done using a DES (3.5x23mm) with final good result. A cardiac CT was done following PCI which confirmed the angiographic findings and found normal subpulmonic non-malignant course of left branch vessel (Lipton's class R II A).



Case Summary
Anomalous origin of left coronary artery from right aortic sinus as a common trunk is very rare. Percutaneous coronary intervention in such anomalies is scarcely reported. We are presenting such a very rare case of percutaneous coronary intervention in a single coronary artery arising from RCC with non-malignant course (Lipton's class R II A). Cannulation and PCI in such anomalous vessel are challenging and increase the technical complexity of the procedure. Meticulous care is needed to avoid injury to the common origin while cannulating as it can lead to catastrophe. Fortunately, in our case, we could cannulate the vessel with JR guiding catheter and complete the procedure successfully.