Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251011_005
Sequential Balloon Dilation With Steerable Sheath in a Challenging Case With Severe Rheumatic Mitral Valve Stenosis
By Jian Kuan Yeh, Mu-Shiang Huang
Presenter
Jian Kuan Yeh
Authors
Jian Kuan Yeh1, Mu-Shiang Huang1
Affiliation
National Cheng Kung University Hospital, Taiwan1
View Study Report
CASE20251011_005
Structural - Other Structural Interventions
Sequential Balloon Dilation With Steerable Sheath in a Challenging Case With Severe Rheumatic Mitral Valve Stenosis
Jian Kuan Yeh1, Mu-Shiang Huang1
National Cheng Kung University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
This is a 58-year-old woman with hypertension. She presented with dyspnea on exertion for several years, which progressed since one year ago, accompanied with paroxysmal nocturnal dyspnea. Physical exam showed clear breath sounds bilaterally, regular heart beats, and a grade III low-pitched diastolic murmur over the apex.
Relevant Test Results Prior to Catheterization
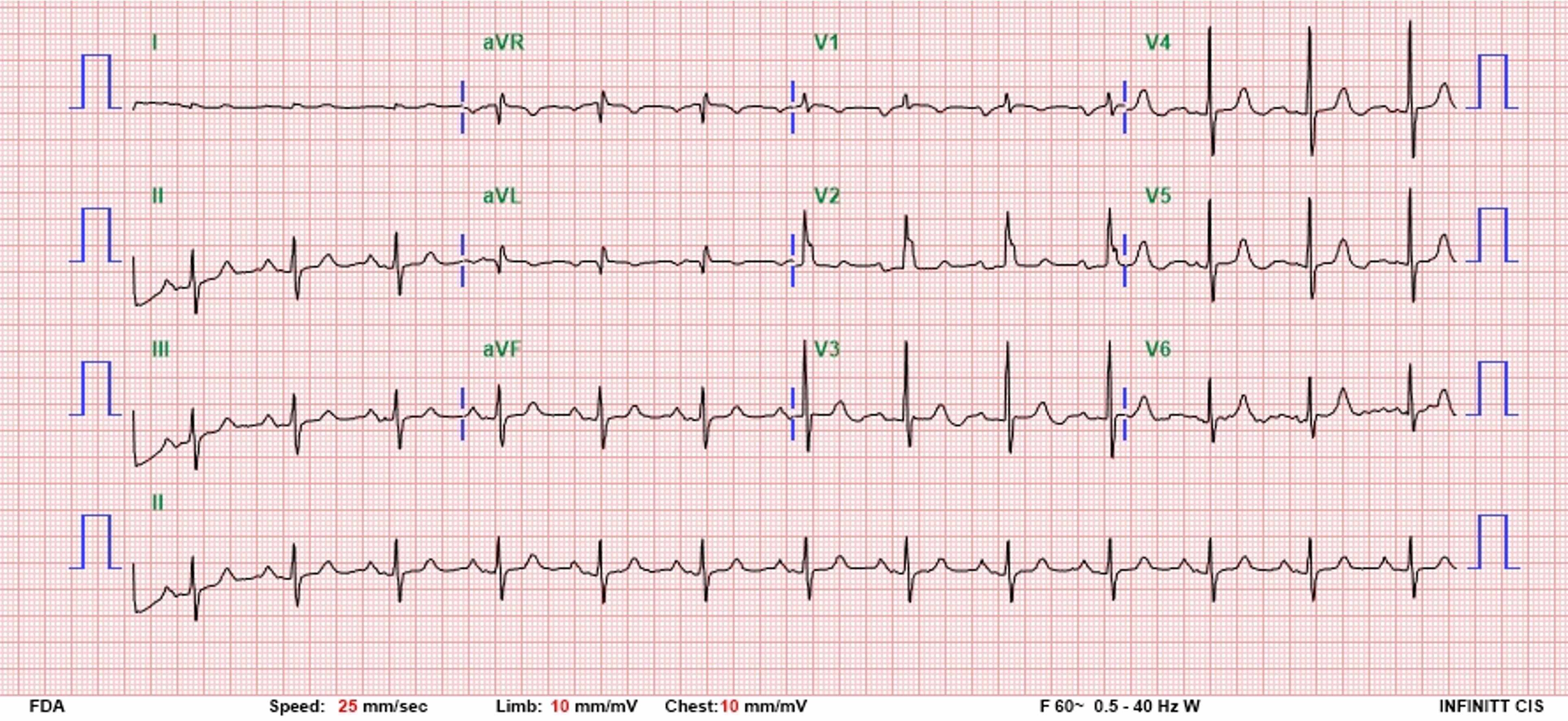
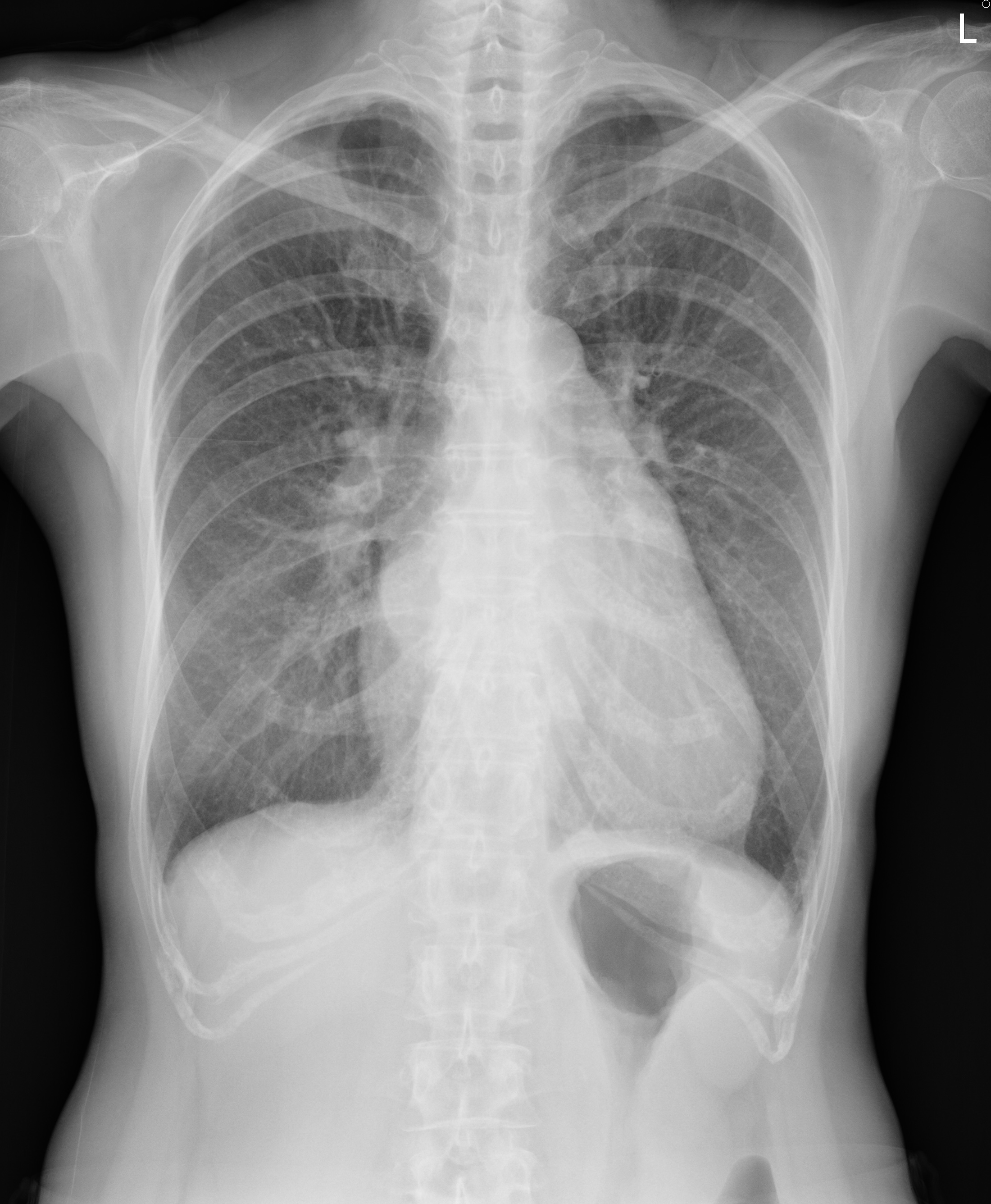
The ECG showed sinus rhythm, first degree AV block, and bi-atrial enlargement. The chest radiograph showed left atrial enlargement with double contour sign. Trans-thoracic echocardiography showed dilated left atrium, adequate global LV systolic function, moderate pulmonary hypertension (estimated PASP 64 mmHg). Commissural fusion and diastolic doming of mitral valve leaflets were present. The mitral valve area was measured 1.03 cm^2, compatible with severe rheumatic mitral stenosis.

 PLAX.mp4
PLAX.mp4
PSAX at MV level.mp4
A4C.mp4
Relevant Catheterization Findings
Trans-esophageal echocardiography showed severe mitral stenosis with mitral valve area measuring 0.689 cm^2 by 3D planimetry. No left atrial appendage thrombus was observed. The Wilkins score was calculated as 7. The patient was admitted for PTMC due to symptomatic severe rheumatic mitral stenosis with favorable anatomical and clinical characteristics.

TEE bicommissural view.mp4
TEE 3D MV.mp4
Interventional Management
Procedural Step
1st procedure:1. Trans-septal puncture with a BRK1 needle.2. Sentinel cerebral protection device deployed.3. Failed passing of the Inoue balloon past the mitral valve (MV).4. 0.035" hydrophilic wire direct wired to the LV, externalized by the EN snare. The Inoue balloon still can not pass through the MV.5. Dilation of the MV with over-the-wire (OTW) balloons (6.0mm, 10.0mm). The Inoue balloon still can not pass through the MV. The first procedure terminated due to prolonged procedure time.2nd procedure:1. Trans-septal puncture with a BRK1 needle. Sentinel cerebral protection device deployed. A temporary pacemaker placed via right IJV for possible rapid pacing during PTMV.2. Direct wiring to the LV using the hydrophilic wire in the steerable sheath. The wire then changed to the Amplatz super stiff 0.035" J-tipped wire for extra support.3. Dilation of the MV with 10.0mm OTW balloon.4. The 24mm Inoue balloon passed through the MV with the distal balloon partially inflated.5. The 24mm Inoue balloon inflated at the MV multiple times.6. The final echocardiogram confirmed lowering of the trans-mitral mean pressure gradient and no pericardial effusion.


Wiring to LV.mp4
Inoue balloon past MV.mp4
PTMV.mp4
Case Summary
1. In patients with large left atrium and relatively small left ventricle, the Inoue balloon may be difficult to pass through the mitral valve due to poor coaxiality.2. Sequential dilation with over-the-wire balloons with the guidance of a steerable sheath may help facilitate the final Inoue balloon dilation. 3. Partially inflating the distal end of the Inoue balloon may facilitate passing of the balloon through the mitral valve.