Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251007_003
Navigating Through the Uncrossable CTO Lesion
By Apichai Marsukjai
Presenter
Apichai Marsukjai
Authors
Apichai Marsukjai1
Affiliation
Charoenkrung Pracharak Hospital, Thailand1
View Study Report
CASE20251007_003
Coronary - Complex PCI - CTO
Navigating Through the Uncrossable CTO Lesion
Apichai Marsukjai1
Charoenkrung Pracharak Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A-70-year-old male with underlying disease of hypertension, dyslipidemia, end stage kidney disease on hemodialysis with history of traumatic intracranial hemorrhage was admitted due to atypical chest pain at rest 1 day without history of orthopnea and PND. His blood pressure was 138/73 mmHg, his heart rate was 100 beats per minute. The physical examinations were unremarkable.
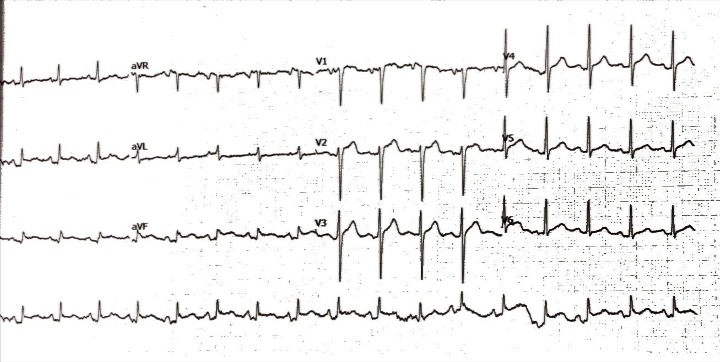
Relevant Test Results Prior to Catheterization
The initial electrocardiogram showed a sinus rhythm rate of 100 beat per minute with ST elevation in II, III and aVF. The transthoracic echocardiography demonstrated a left ventricular ejection fraction of 58% with inferior wall hypokinesia with no significant valvular abnormalities.
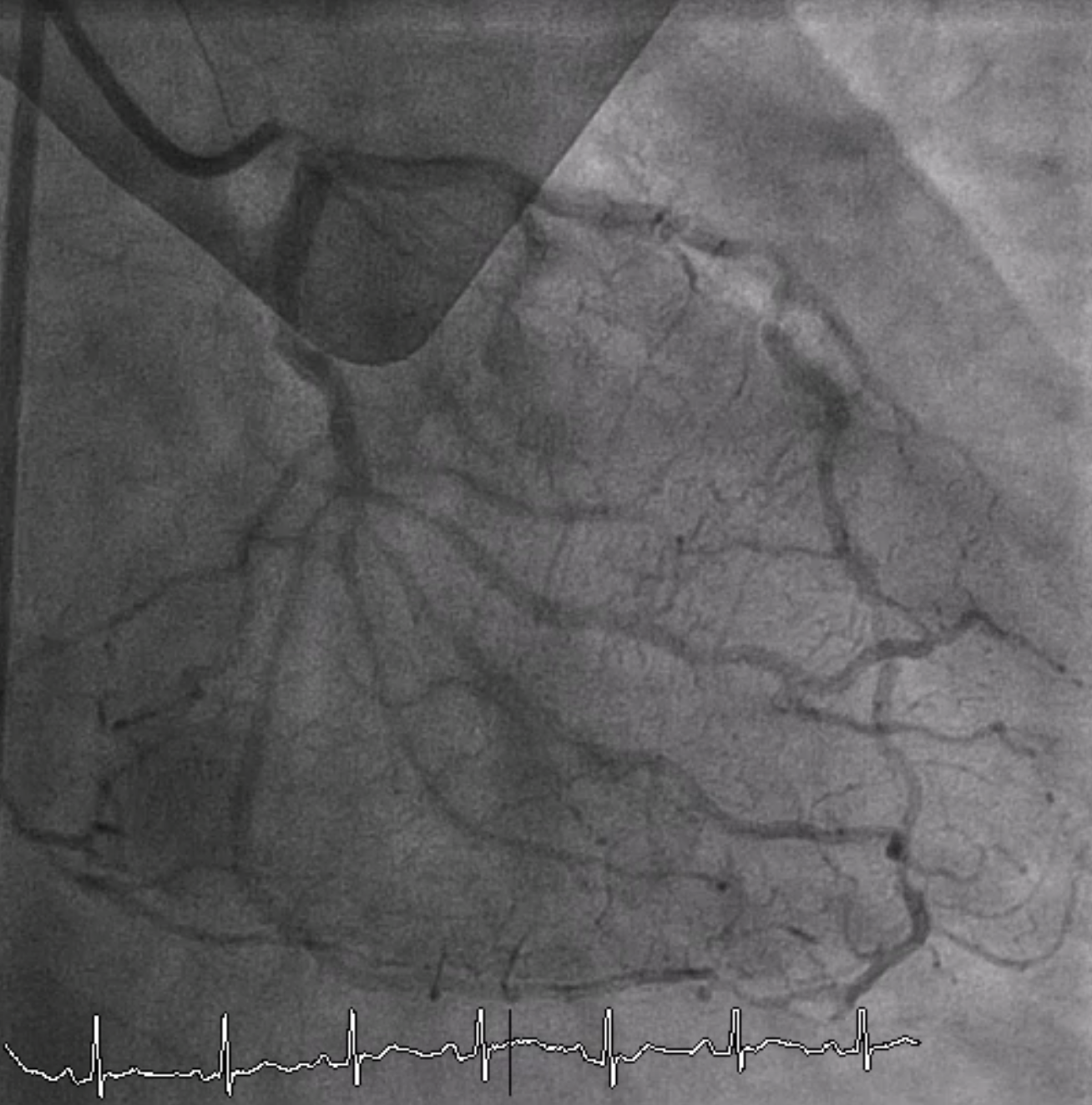
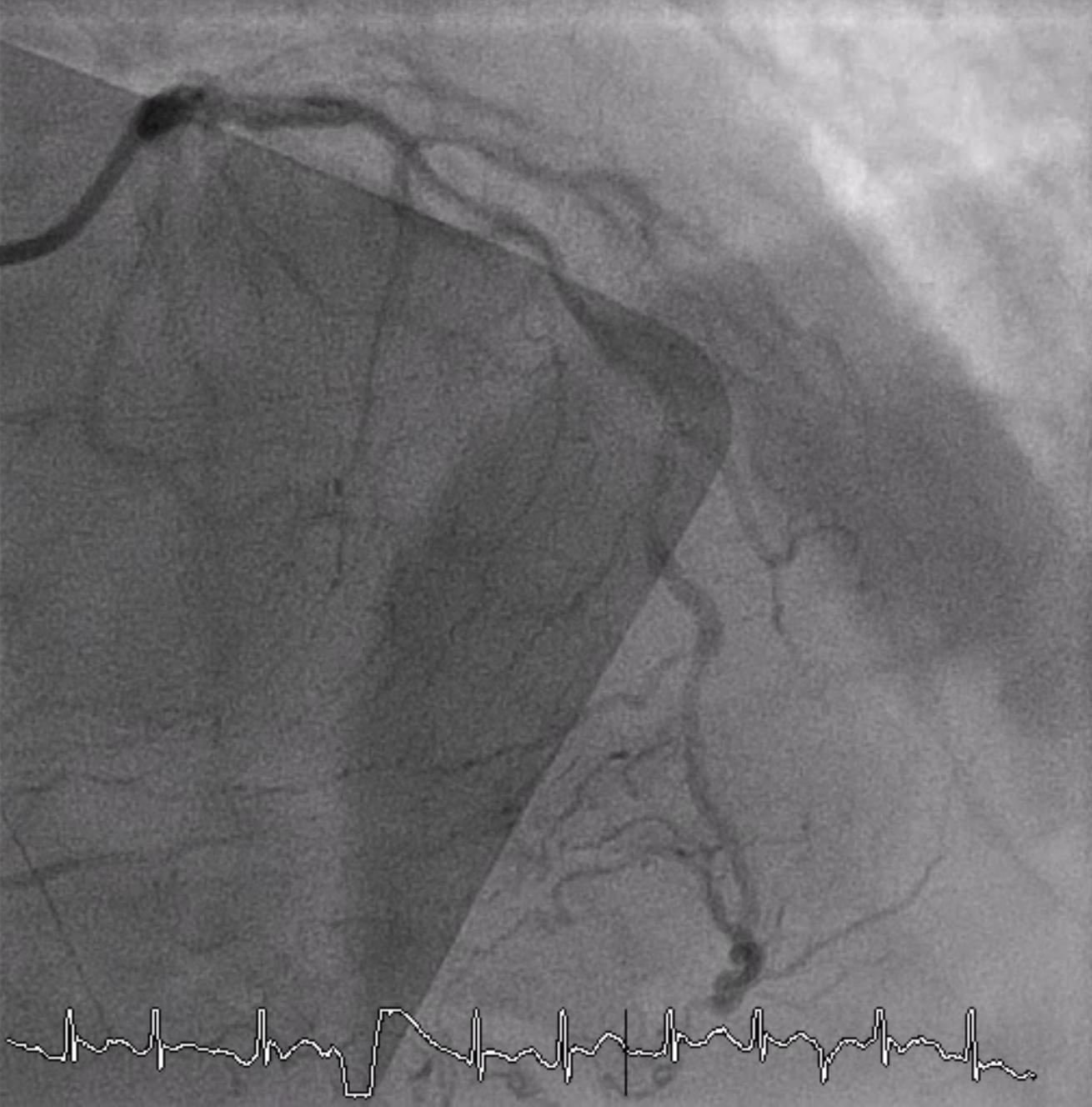
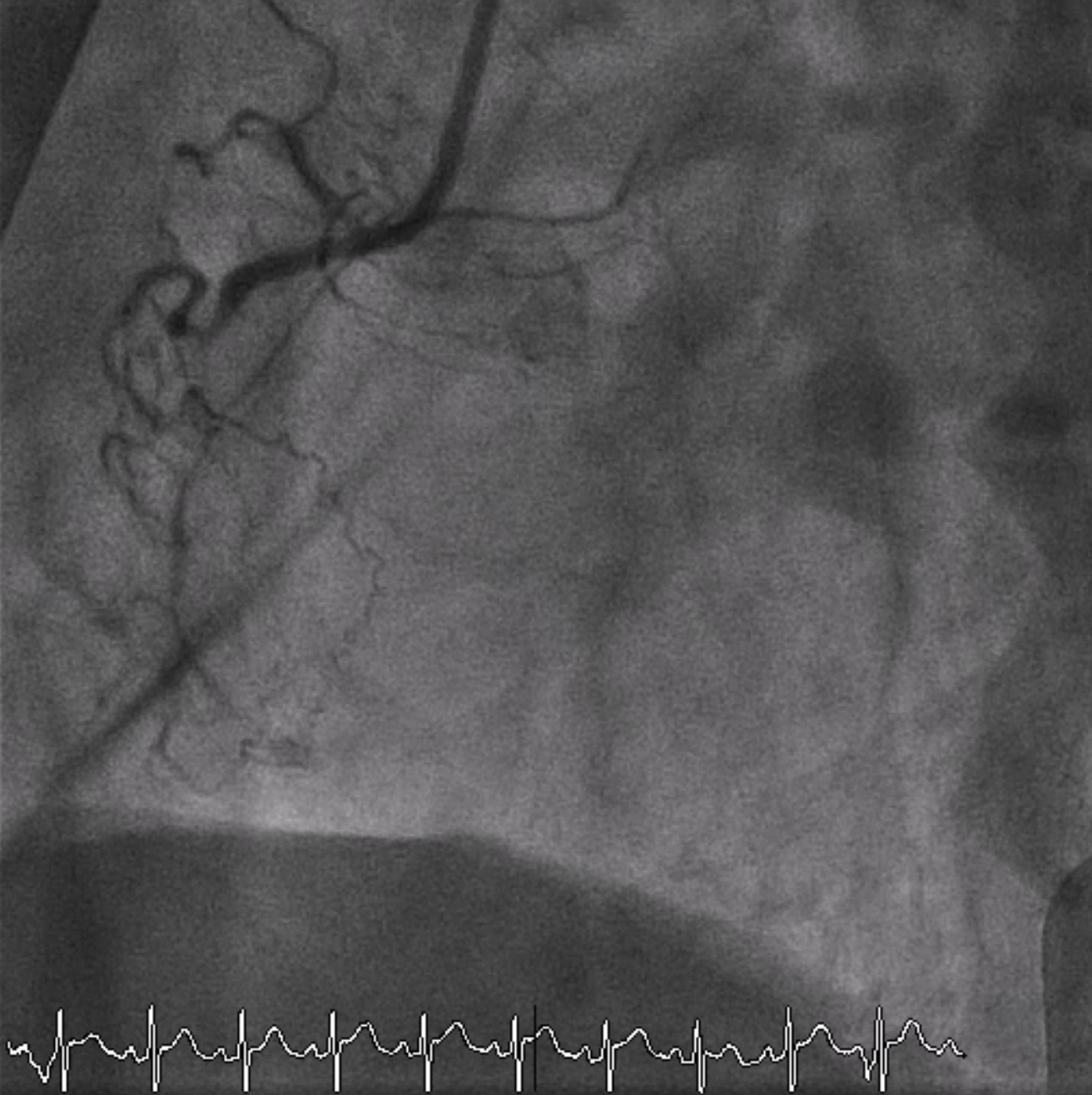
Relevant Catheterization Findings
Coronary angiography revealed total occlusion at proximal RCA with collateral circulation from conus branch, LAD and LCx to RCA. 70-80% stenosis at proximal to mid LAD and 50% stenosis at distal Lcx and OM.
 CINE.mp4
CINE.mp4
CINE 1.mp4
CINE 2.mp4
Interventional Management
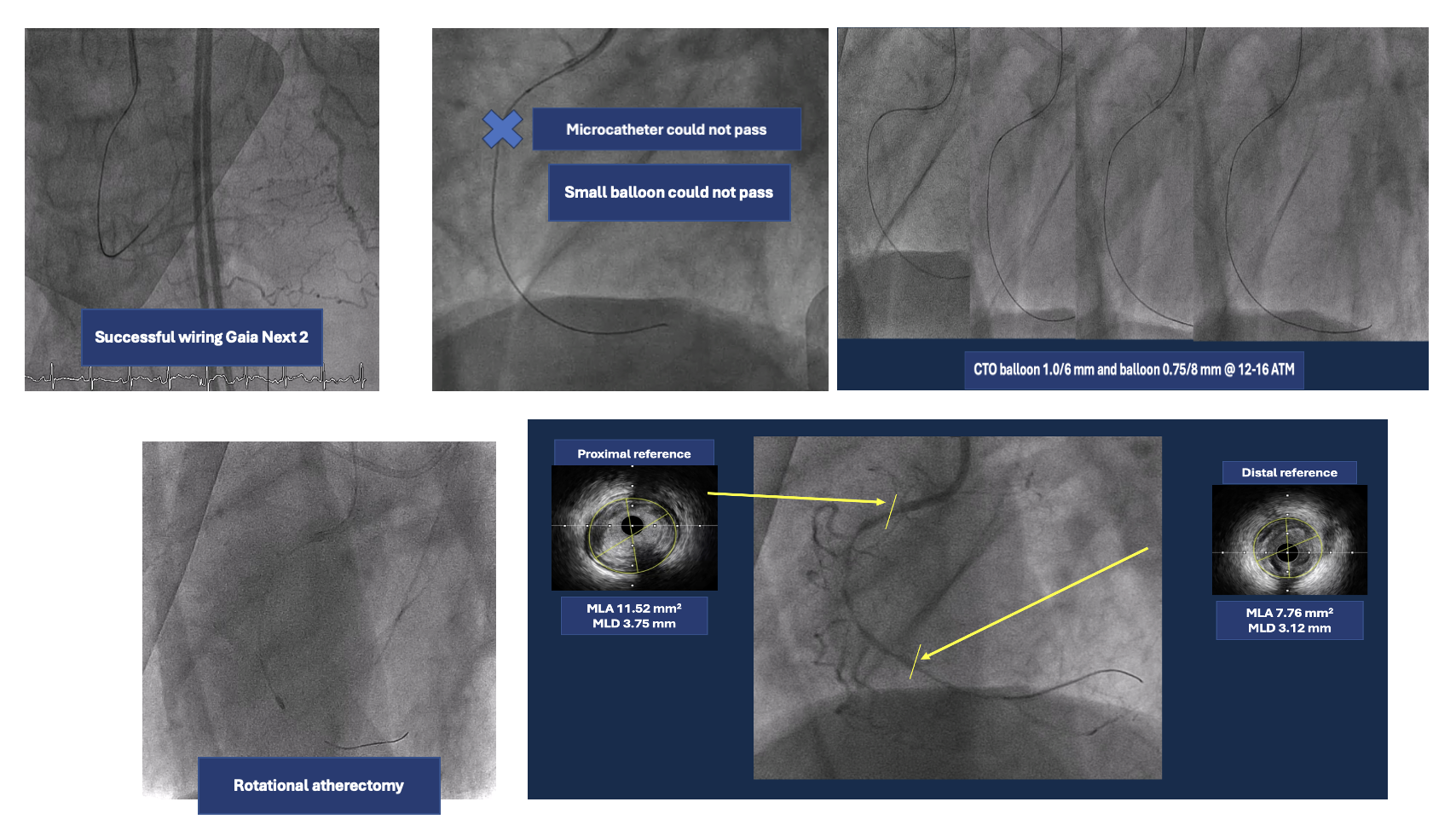
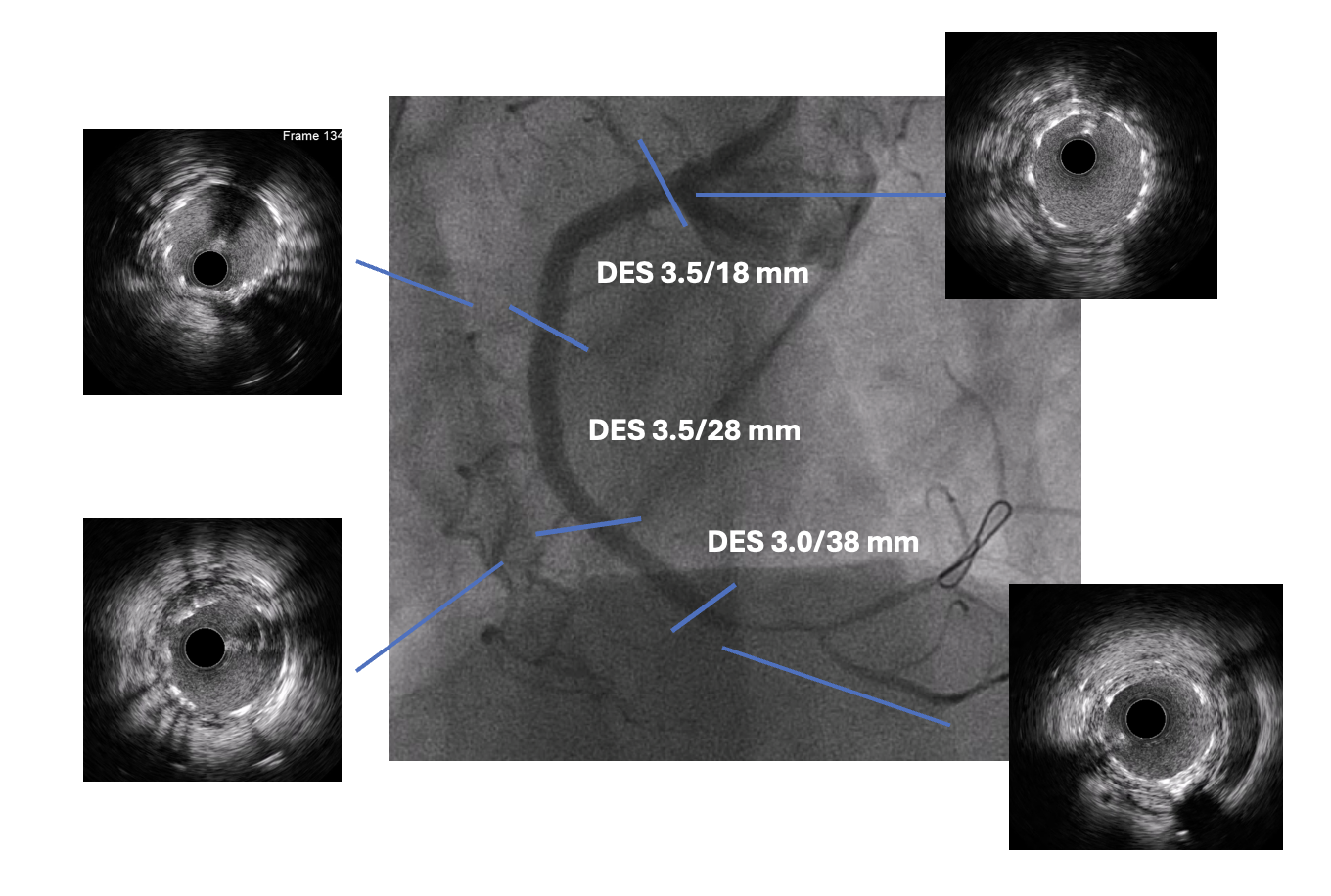
Procedural Step
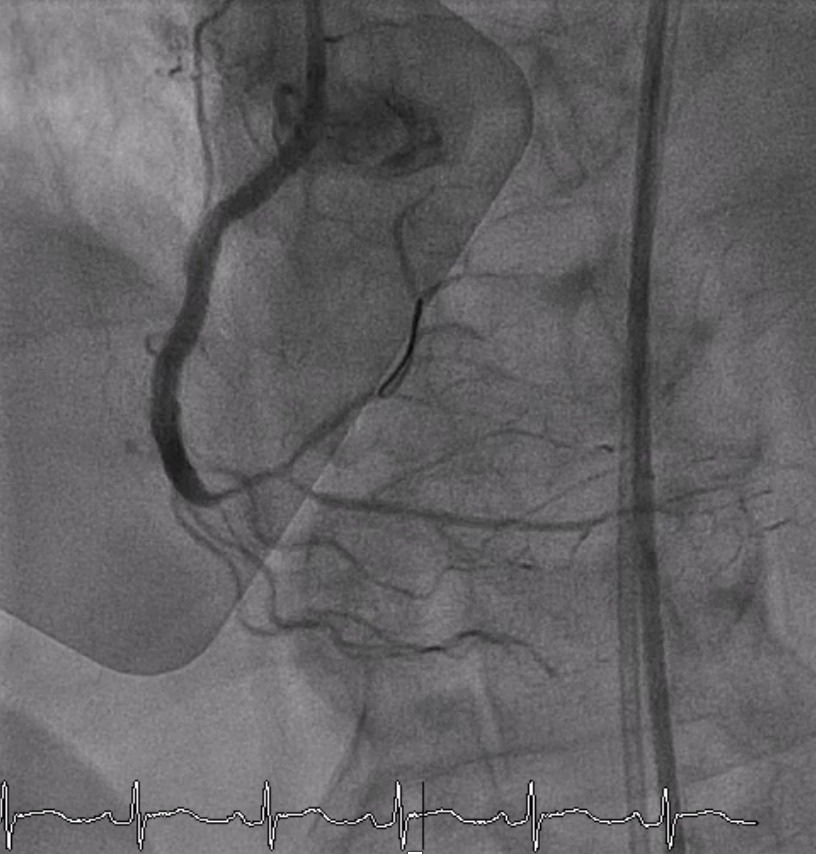
A 6 Fr JR 4.0 guiding catheter was engaged via femoral approach and JL 4 catheter was used for dual injection. We planned to perform PCI at proximal RCA CTO with antegrade wire escalation technique first. We successful wired to PL branch of RCA using microcatheter with Gaia Next 2 guidewire (Failed using Fielder XT). The microcatheter could not cross lesion. Try using CTO balloon 0.75/8 mm and 1.0/6 mm to pre-dilatation but still uncrossable. So we put the microcatheter farthest and successful bare wiring the RotaWire Floppy to PL. Rotational atherectomy was done with Burr 1.25 mm at 172,000 - 146,000 rpm total 4 runs. IVUS was pulled back from PL-RCA showed intra-plaque wiring, calcified nodules with cracked calcific plaques and reverberation. We prepared the lesion proximal to mid RCA lesion with non-compliant 2.5/15 mm balloon at 20 atm and scoring 3.0/13 mm balloon at 18-20 atm. A 3.0/38 mm stent could not be delivered the lesion. We used the guide extension catheter with balloon-assisted tracking techinque for delivery. The stent was successfully deployed to mid RCA. The 3.5/28 mm stent was deployed to proximal to mid RCA and 3.5/18 mm stent was deployed at ostial RCA. Post-dilatation with non-compliant 3.0/15 and 3.5/18 mm at 16 atm. Final angiogram showed good coronary blood flow and IVUS demonstrated well stent expansion, no malapposition and no stent edge dissection.
IVUS first run.mp4
Rotablator.mp4
Final angiogram.mp4
Case Summary
Ad hoc CTO PCI in ACS patient should be carefully discussed. This case demonstrated importance of guiding catheter support and careful analysis of anatomy. Uncrossable lesions remain a challenge, rotational atherectomy could be useful in this situation. Intravascular imaging is also useful in determining strategy and technique for optimizing CTO PCI outcome.