Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251007_002
Breaking Double Barriers
By Tussapon Raomanachai, Thunnop Chotivanawan
Presenter
Tussapon Raomanachai
Authors
Tussapon Raomanachai1, Thunnop Chotivanawan2
Affiliation
Queen Savang Vadhana Memorial Hospital, Thailand1, Thammasat University Hospital, Thailand2
View Study Report
CASE20251007_002
Coronary - Complex PCI - CTO
Breaking Double Barriers
Tussapon Raomanachai1, Thunnop Chotivanawan2
Queen Savang Vadhana Memorial Hospital, Thailand1, Thammasat University Hospital, Thailand2
Clinical Information
Relevant Clinical History and Physical Exam
A 48-year-old male with a history of treated pulmonary tuberculosis resulting in a destroyed right lung, end-stage renal disease on regular hemodialysis was admitted with non-ST-elevation ACS complicated by congestive heart failure with respiratory failure on endotracheal tube. After decongestion, he could extubation and stable without oxygen support. Angiography showed left main disease and double chronic total occlusion. The Heart Team decided to decline CABG and appointed him for stage PCI.
Relevant Test Results Prior to Catheterization
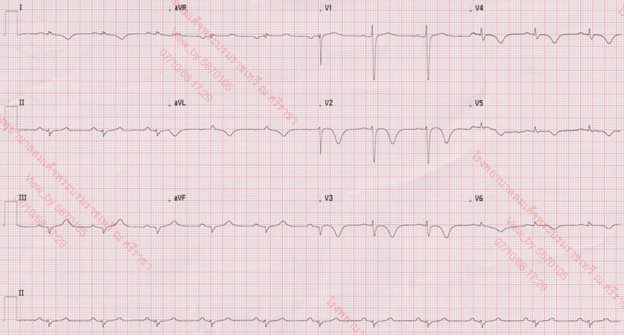
The initial electrocardiogram showed a sinus rhythm rate of 66 beat per minute with new T wave inversion in V2 to V6 and I, aVL. The Chest Xray showed increase CT ratio with pulmonary congestion with visualized endotracheal tube and no significant change of destroyed right lung. The transthoracic echocardiography demonstrated a left ventricular ejection fraction of 33% with anterior and lateral wall hypokinesia from basal to apex and no significant valvular abnormalities.

 Echo _ A4 Pre.mp4
Echo _ A4 Pre.mp4
Echo _ PLAX pre.mp4
Echo _ PSAX pre.mp4
Relevant Catheterization Findings
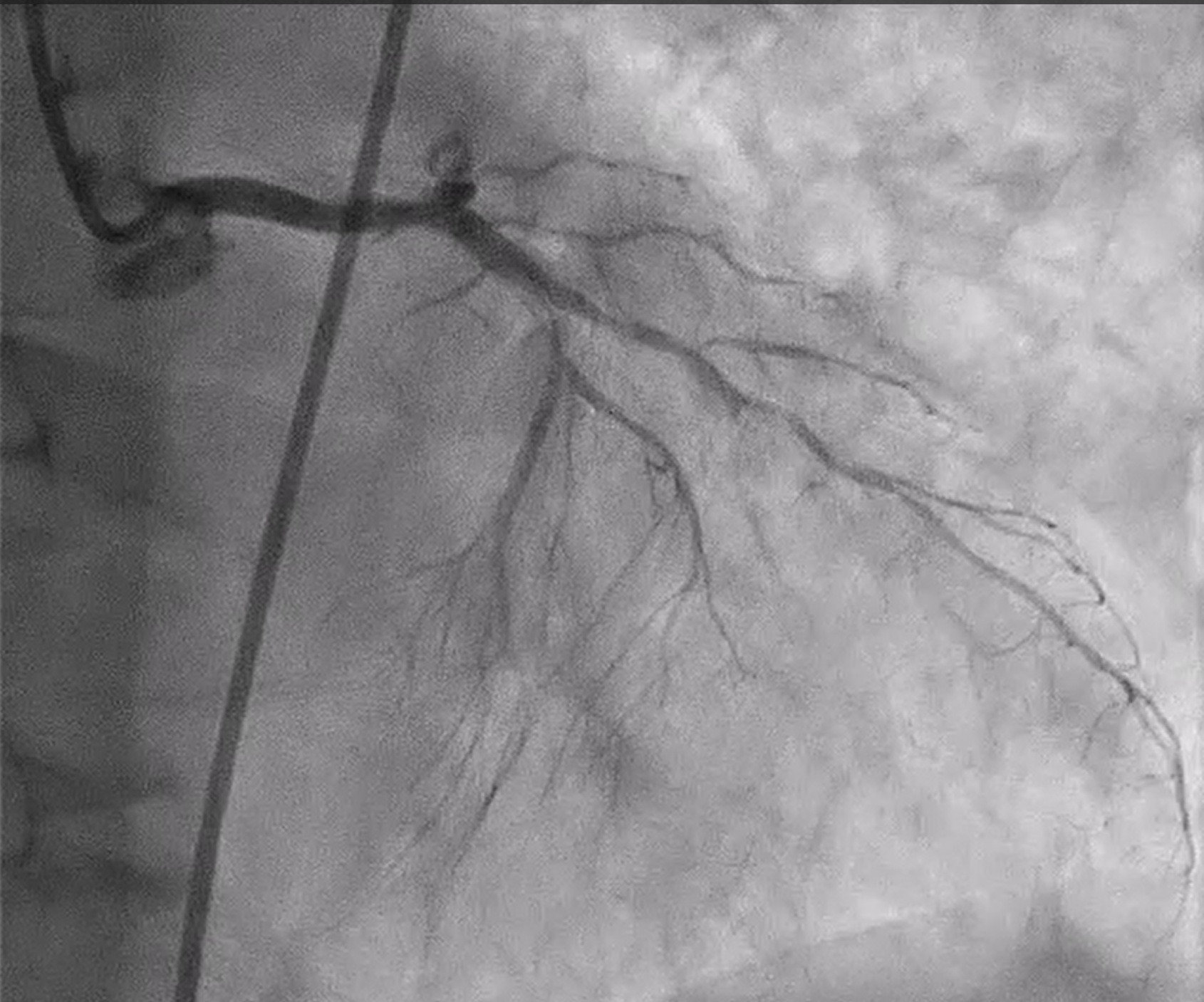
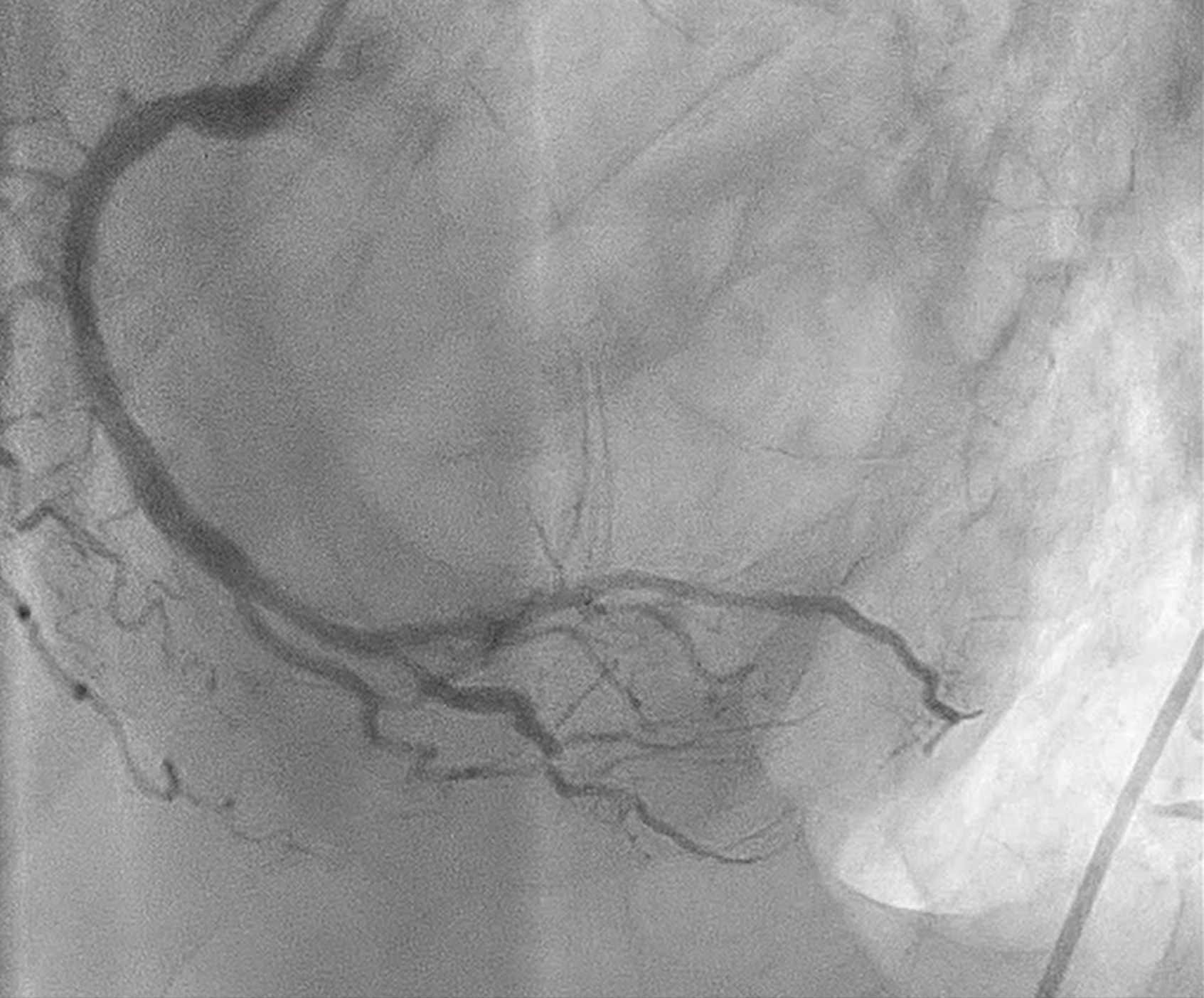
Coronary angiography revealed heavily calcified along LM, proximal to mid LAD, LCx and proximal RCA. 50% stenosis at distal LM bifurcation (Medina 1-1-0). 70% stenosis at proximal LAD and total occlusion at mid LAD. Total occlusion at proximal LCx. No significant stenosis of RCA. There were collateral circulations from septal branch of LAD to distal LAD and from PL to distal LAD and distal LCx.

RAO CRA.mp4
RAO CAU contralat.mp4
LAO RCA.mp4
Interventional Management
Procedural Step
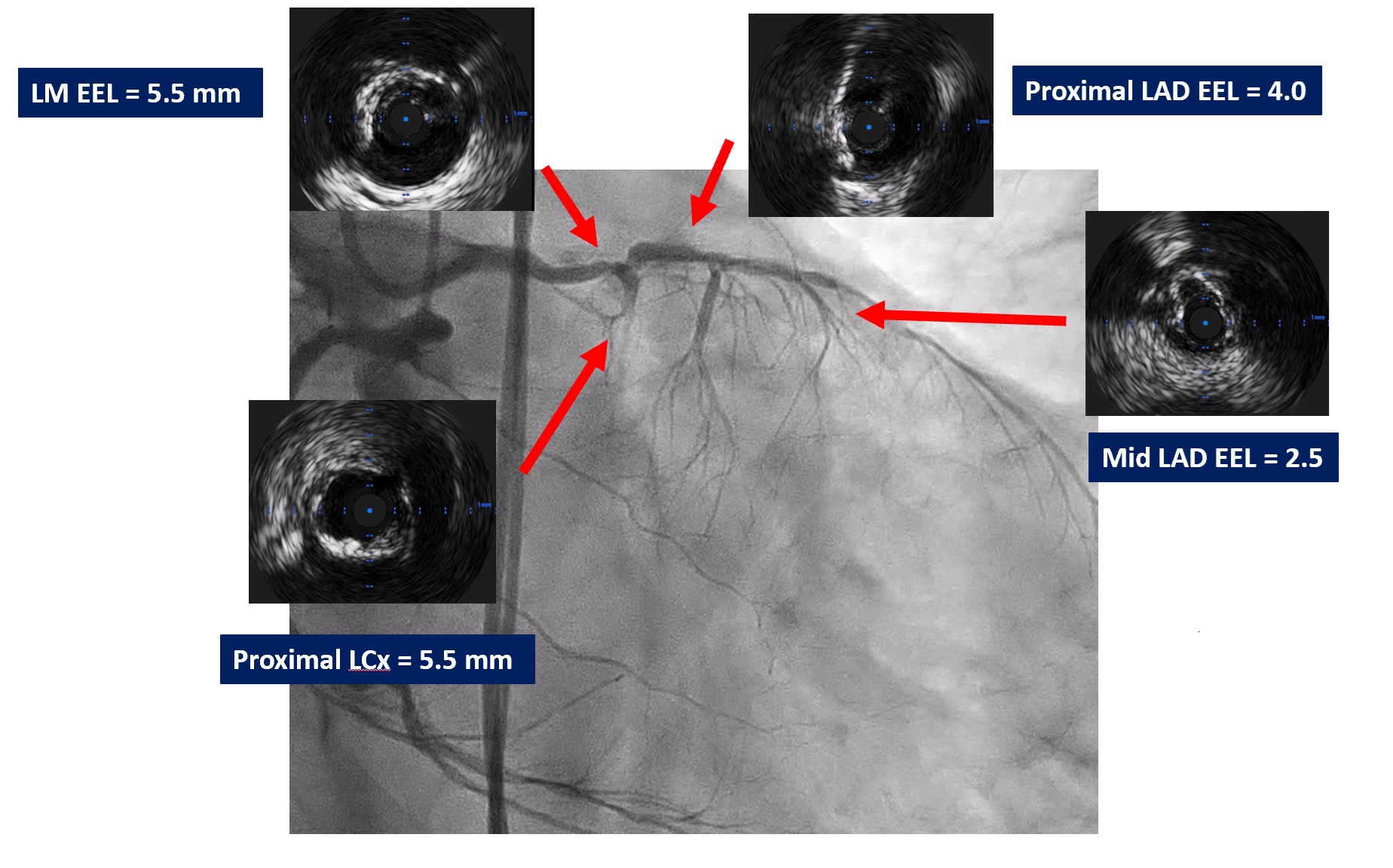
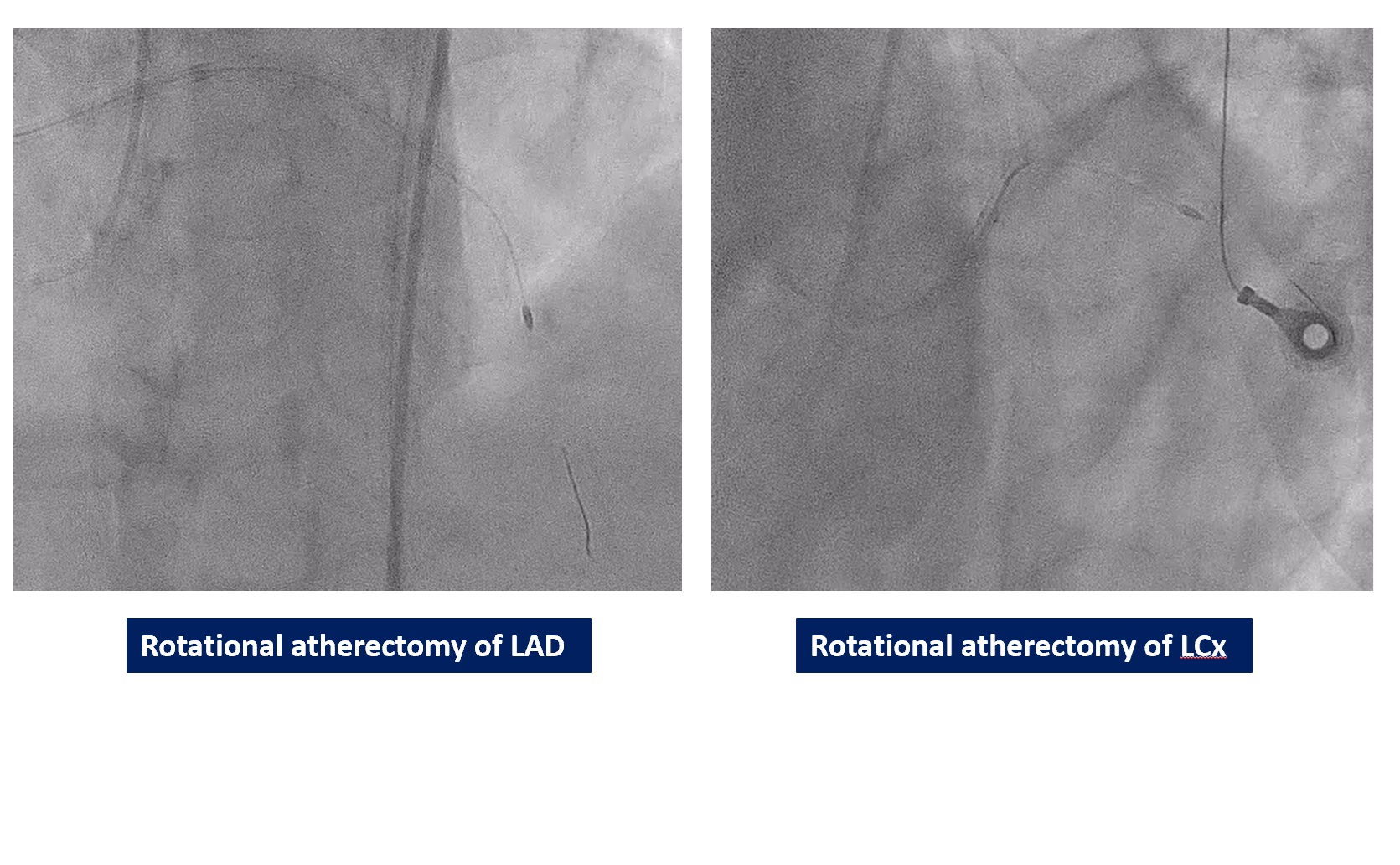
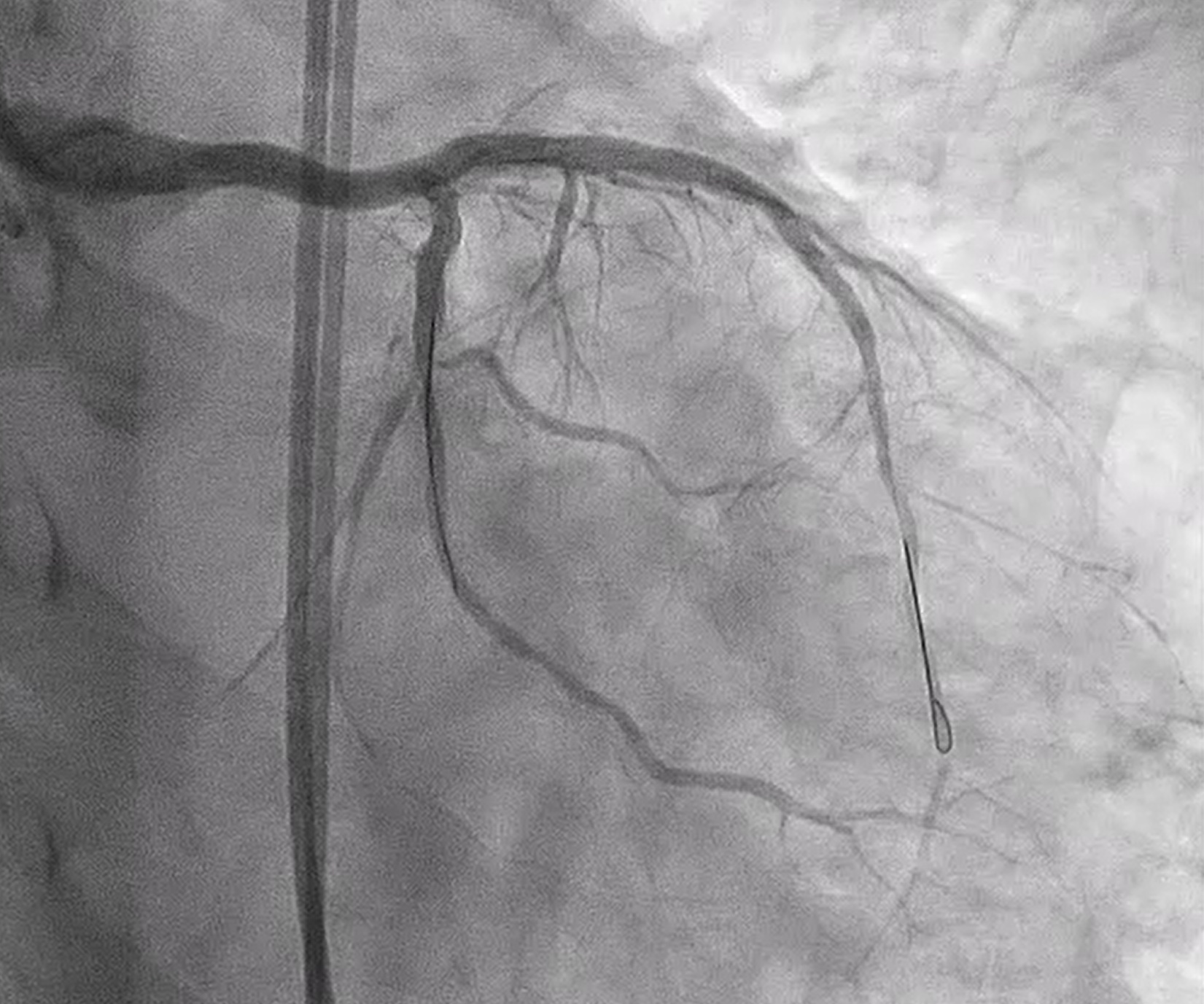
We performed PCI at CTO LAD and LCx with contralateral injection with antegrade wiring and upfront rotablation at LM, LAD and LCx due to heavily calcified lesion. The 7 Fr EBU 3.5 and 6 Fr JR 4.0 catheter were engaged into LCA and RCA, respectively. We opened the LCx CTO segment using microcatheter with Fielder XT guidewire (GW) then rewire from LCx to distal LAD. The CTO GW was exchange to RotaWire Floppy. Rotablation was done at LM-mid LAD with Burr 1.5 mm and LM-proximal LCx with Burr 1.5 mm. IVUS showed EEL of mid LAD = 2.5 mm, proximal LAD = 4.0 mm, distal LM = 5.5 mm and proximal LCx = 3.5 mm. The lesion of mid LAD was prepared with scoring balloon 2.0/15 mm and LM-proximal LAD with scoring balloon 3.5/15 mm. A 2.5/33 mm stent was deployed from proximal-mid LAD. We decided to stenting the lesion at proximal LCx before stenting the lesion at LM-proximal LAD using provisional one stent and POT-kiss-POT technique. A 3.0/26 mm stent was deployed at proximal LCx. A 3.5/38 mm stent was deployed from distal LM-proximal LAD and 3.5/13 mm stent from ostial LM-distal LM. POT was done with a non-compliance (NC) 5.0/12 mm balloon along LM stent. Kissing balloon inflation with NC 3.0/15 mm balloon at LM-LCx and 3.5/15 mm balloon at LM-LAD then final POT with NC 5.0/12 mm was done. IVUS showed well stent expansion, no malapposition and no stent edge dissection. The patient had no re-admission. Echocardiography after 3 months showed significant improvement of LV function to 56%.
CINE final A.mp4
CINE final C.mp4
IVUS post.mp4
Case Summary
The primary treatment for complex coronary artery disease was traditionally coronary artery bypass graft (CABG) surgery. However, complex percutaneous coronary intervention (PCI) is now a feasible option that can achieve good results, especially in patients who are unsuitable for surgery. This case successfully demonstrates a highly complex PCI used to treat a double chronic total occlusion (CTO). The procedure, which involved rotational atherectomy of both the LAD and LCx arteries in a high-risk patient, achieved excellent results without any complications, thus confirming the utility of advanced PCI strategies.