Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251005_001
Stone Crusher Symphony: Triple Device Harmony in Complex PCI
By Andy Sukmadja, Gavin Ng
Presenter
Andy Sukmadja
Authors
Andy Sukmadja1, Gavin Ng2
Affiliation
Ng Teng Fong General Hospital, Singapore1, National University Hospital, Singapore2
View Study Report
CASE20251005_001
Coronary - Complex PCI - Calcified Lesion
Stone Crusher Symphony: Triple Device Harmony in Complex PCI
Andy Sukmadja1, Gavin Ng2
Ng Teng Fong General Hospital, Singapore1, National University Hospital, Singapore2
Clinical Information
Relevant Clinical History and Physical Exam
A 66 year old man with end stage renal failure was consulted due to intradialytic chest pain. Patient also has long standing history of diabetes, hypertension, dyslipidemia and bilateral below knee amputation. Cardiomegaly was noted during physical examination. ECG showed ST depression on anterolateral lead.
Relevant Test Results Prior to Catheterization
Serial troponin increased from 11254 ng/L to 34188 ng/L. Transthoracic echocardiography showed left ventricular hypertrophy and preserved Ejection Fraction.
Relevant Catheterization Findings
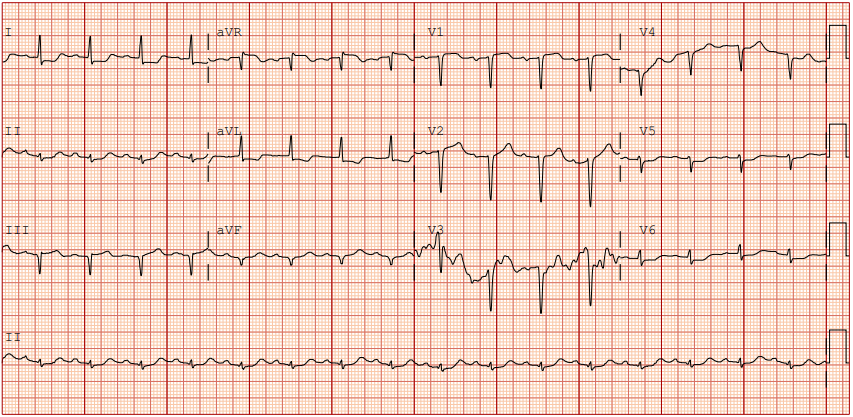
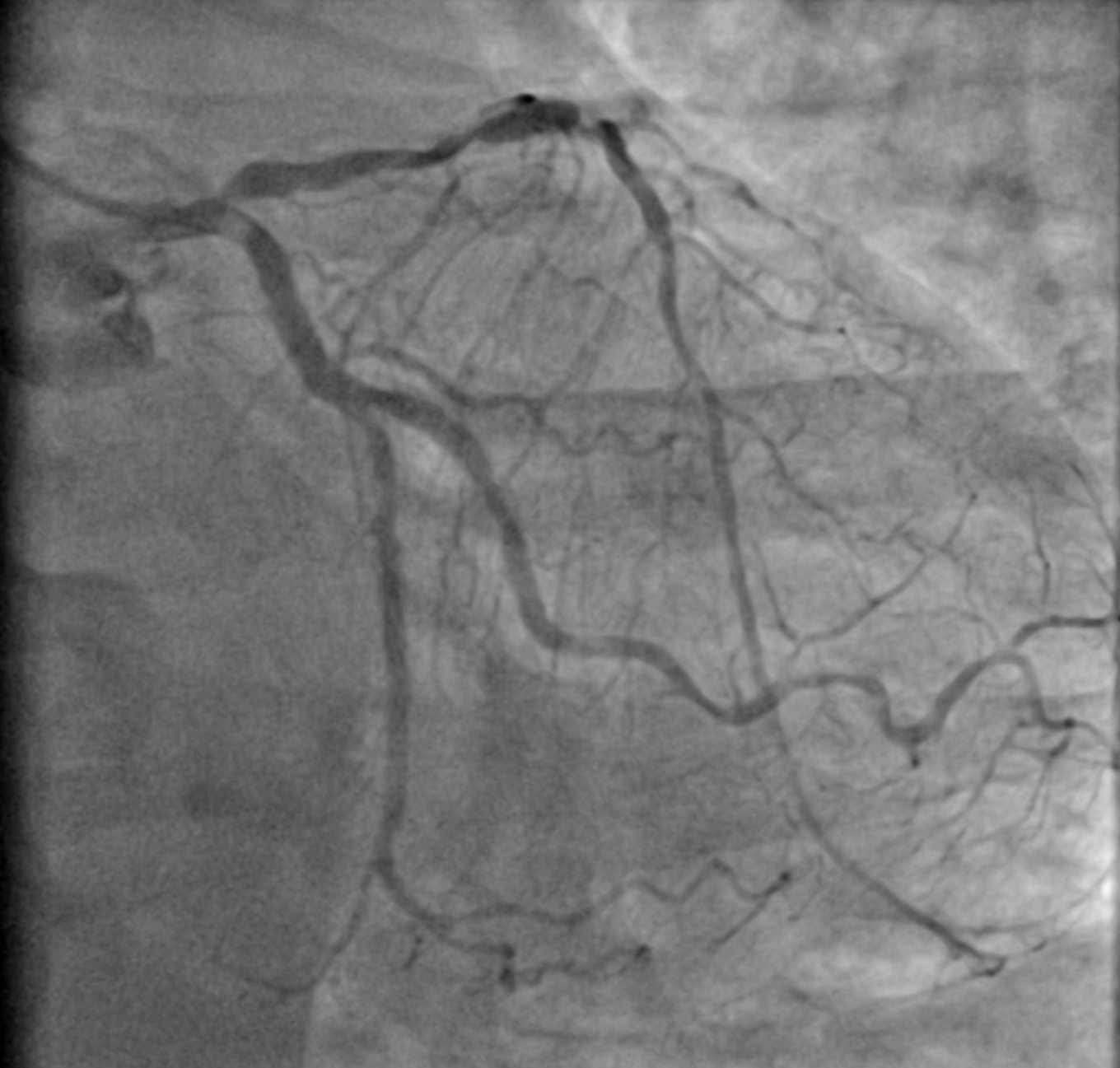
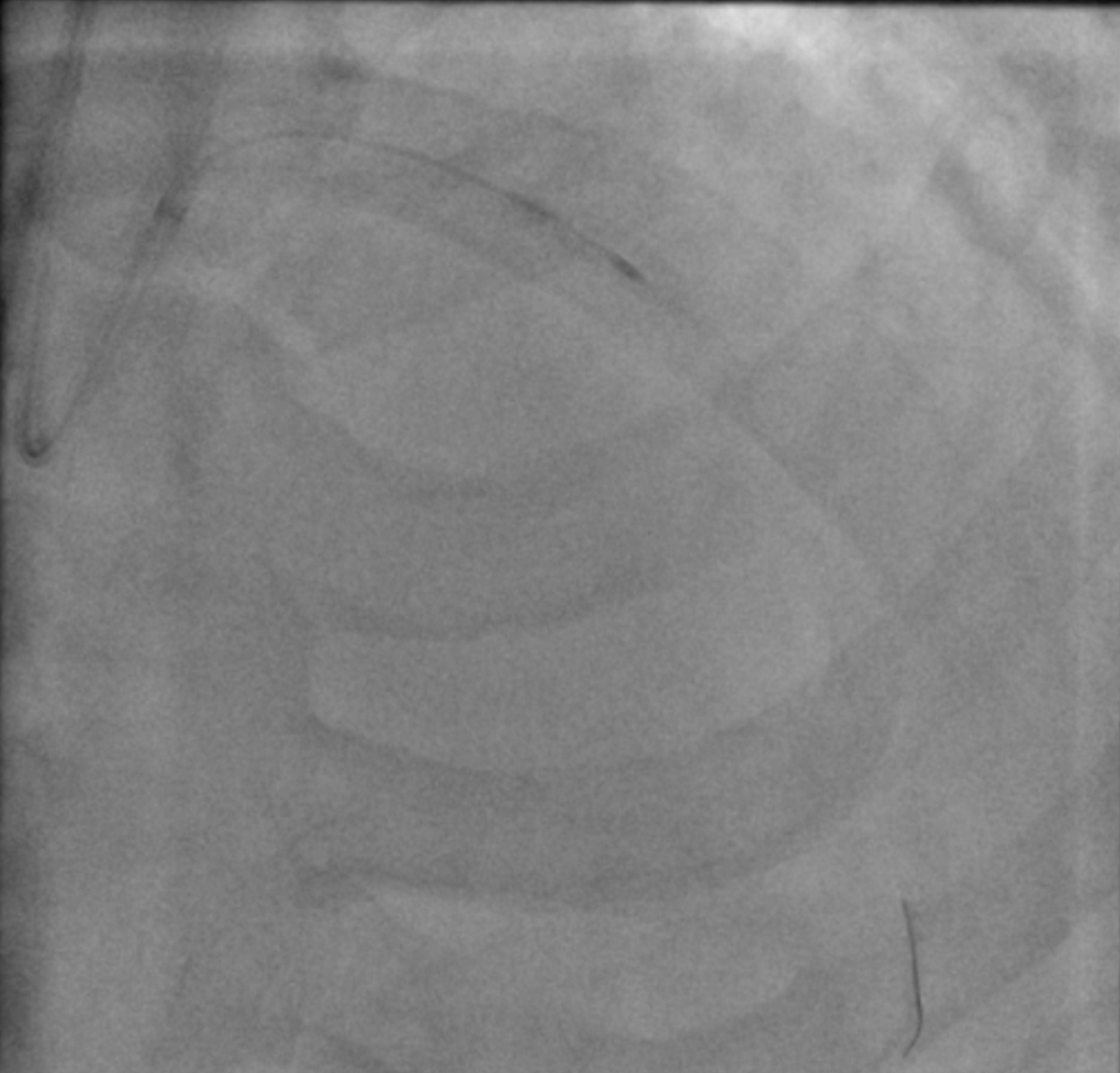
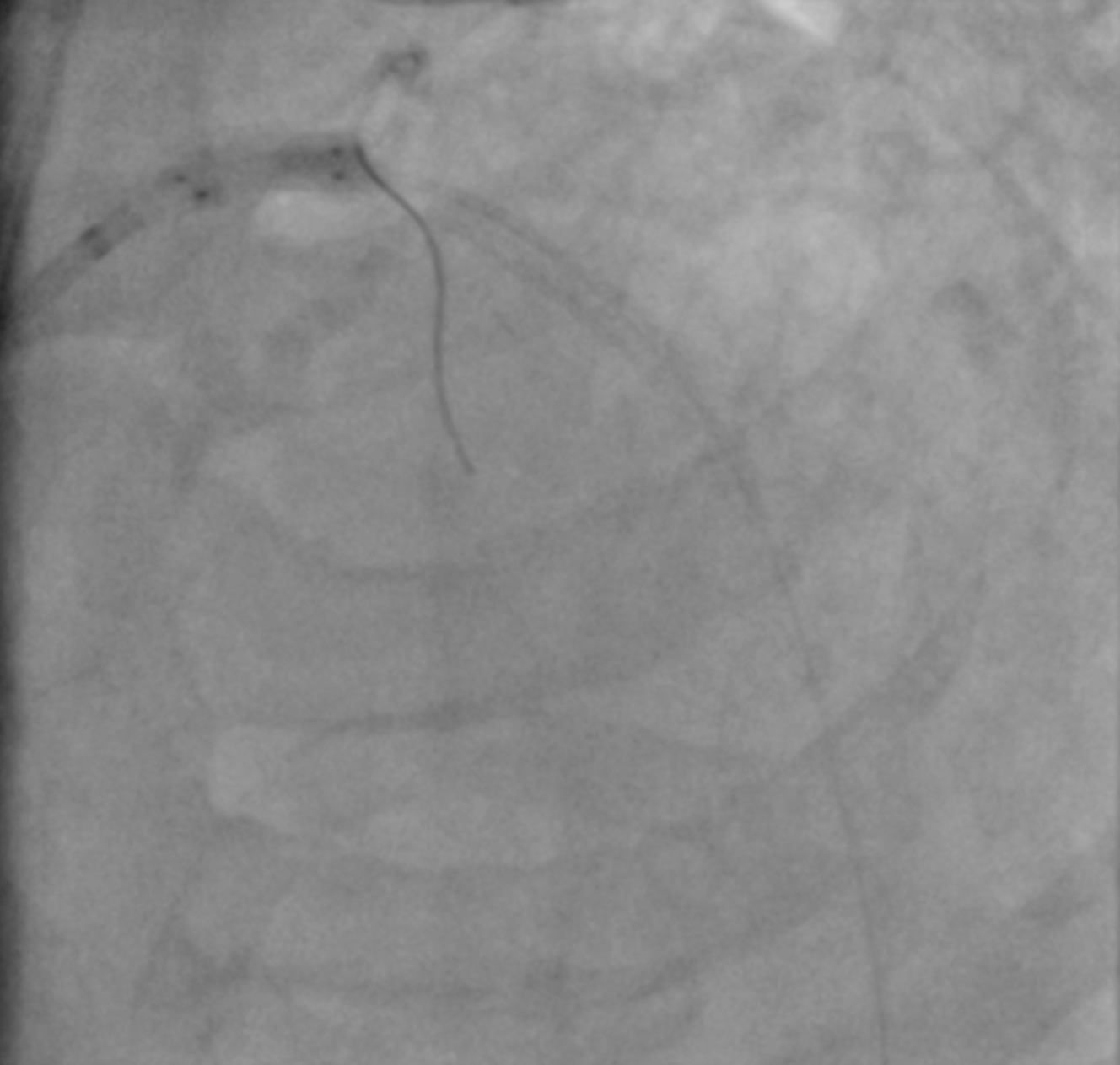
Angiography showed triple vessel disease involving LM-LAD-LCx bifurcation with eccentric calcium nodule in the ostial LCx. Severe calcification was noted throughout the proximal to mid LAD with some focal severe stenosis. RCA showed one area of severe focal stenosis.

 1 rao cau .mp4
1 rao cau .mp4
2 ap cra.mp4
RCA.mp4
Interventional Management
Procedural Step
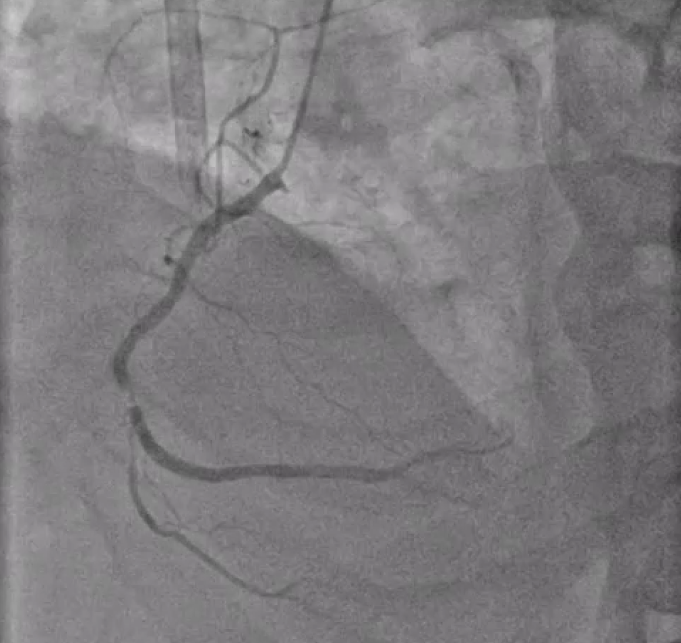
We decided to do orbital atherectomy to ostial LCx and rotational atherectomy to proximal - mid LAD. Calcium debulking was confirmed with IVUS after atherectomy. Subsequent predilation using high pressure scoring balloon in LAD failed to obtain sufficient expansion, hence we decided to use intravascular lithotripsy to further modify the calcium throughout proximal LAD. After obtaining optimal balloon expansion, we proceeded with DK crush to LM-LAD-LCx bifurcation. Dual lumen microcatheter was used to facilitate wire recrossing and ensuring wire would stay in true lumen. After final POT in LM, Repeat IVUS was performed to confirm optimal stent expansion. Suboptimal distal stent landing zone due to diffusely diseased LAD was noted and decision was made to angioplasty the distal LAD with Drug Coated Balloon.
6 orbita cx.mp4
9 rota LAD.mp4
25 final rao cau.mp4
Case Summary
Severe coronary calcium remains a major adversary in interventional cardiology, increasing procedural complexity and compromising long-term outcomes. Effective plaque modification with the optimal device—or combination of devices—is crucial to achieve adequate stent expansion, optimize luminal gain, and reduce the risk of future target vessel revascularization. This case highlights how tailoring calcium treatment strategies can turn an otherwise formidable lesion into a predictable and durable PCI result.