Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251004_002
A Case of Complete Revascularization in a Patient With 3-Vessel Disease and Underlying Colon Malignancy Undergoing Major Operation
By Kee Wei Lee, Syed Saleh Syed Sheikh, Alexander Loch, Ramesh Singh Arjan Singh
Presenter
Kee Wei Lee
Authors
Kee Wei Lee1, Syed Saleh Syed Sheikh1, Alexander Loch1, Ramesh Singh Arjan Singh1
Affiliation
University Malaya Medical Centre, Malaysia1
View Study Report
CASE20251004_002
Coronary - Complex PCI - Multi-Vessel Disease
A Case of Complete Revascularization in a Patient With 3-Vessel Disease and Underlying Colon Malignancy Undergoing Major Operation
Kee Wei Lee1, Syed Saleh Syed Sheikh1, Alexander Loch1, Ramesh Singh Arjan Singh1
University Malaya Medical Centre, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 65-year old male, with background history of diabetes mellitus, hypertension and atrial fibrillation on dabigatran, presented with 2-month history of constipation associated with left iliac fossa (LIF) pain. He was diagnosed as having sigmoid adenocarcinoma with no distant metastasis after extensive work-up in Surgical ward. Physical examination was unremarkable other than non-specific LIF tenderness and mild conjunctival pallor. His vitals were stable.
Relevant Test Results Prior to Catheterization
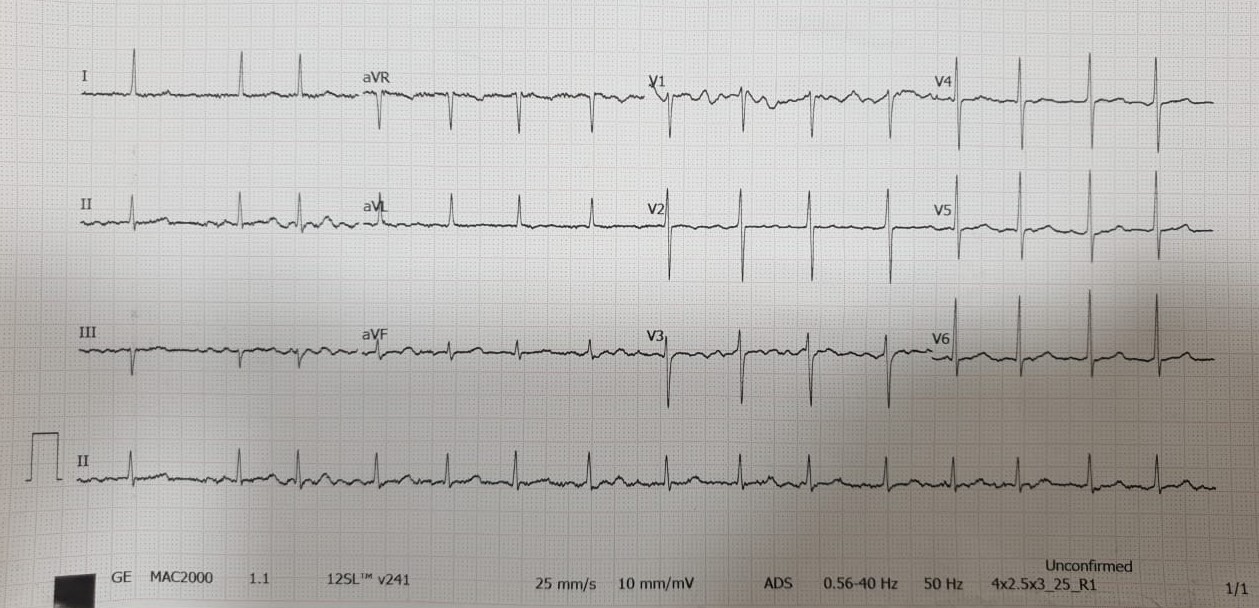
He had microcytic hypochromic anemia with hemoglobin (Hb) of 8.8 g/dL. His renal and liver function tests were normal. Troponin I was not elevated. Electrocardiogram showed rate-controlled atrial fibrillation. 2D-echocardiogram showed LV systolic dysfunction with EF of 37% with hypokinesia at apical and anteroseptal segments. He was planned for tumor resection and was referred for cardiac work-up after a multi-disciplinary discussion between Surgical, Cardiology and Anesthesiology team.
Relevant Catheterization Findings
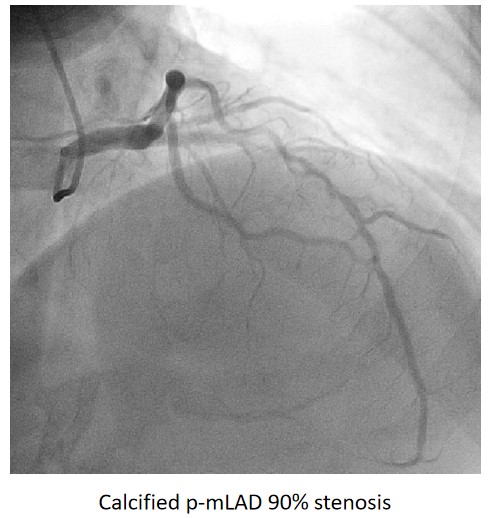
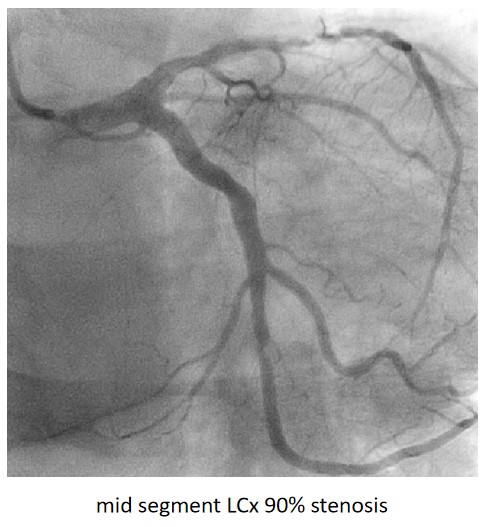
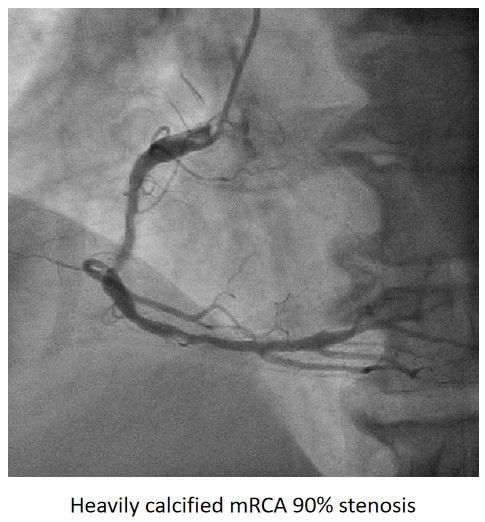
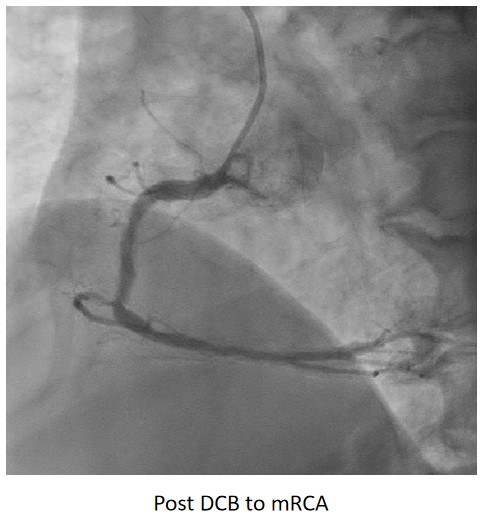
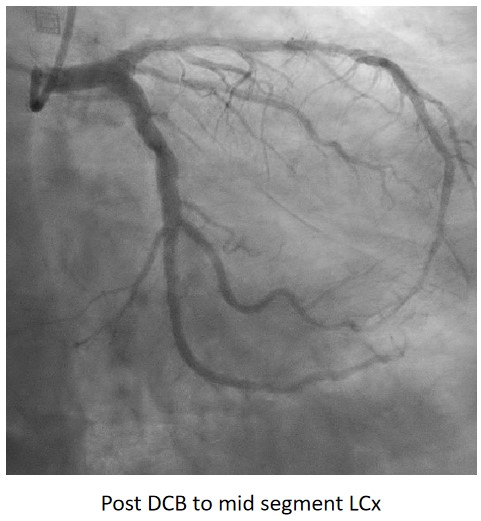
Urgent coronary angiography showed smooth LMCA with severe 3-vessel involvement. There was diffuse LAD lesion with critical stenosis at proximal-to-mid segment. Mid-segment of LCx was 90% stenosed while RCA was heavily calcified with critical stenosis at its mid segment. Our strategy will be complete revascularisation by employing DCB-only strategy.
Interventional Management
Procedural Step
Complete revascularisation was achieved with 2-staged procedures. Up-front plaque modification with rotational atherectomy/IVL with IVUS was planned but limited by patient’s cost constraint. Vascular access obtained with transradial puncture with 6 Fr sheath. Guiding catheter (GC) Judkins Right 4.0 (Cordis, USA) 6 Fr was used to engage right coronary ostium. Runthrough Floppy (Terumo, Japan) wire was wired down RCA. Pre-dilatation balloons were unable to cross the heavily calcified mRCA lesion. Next, GC was changed to Amplatz Left 1.0 (Cordis, USA) for better support and proceeded for further lesion preparation with cutting balloon Wolverine (Boston Scientific, USA) 3.5 x 10 mm and DCB Prevail (Medtronic, USA) 3.0 x 20 mm was deployed. We scheduled him for staged PCI to the left coronaries in 2 weeks time via transradial approach with 6 Fr sheath. GC XB LAD 3.5 (Cordis, USA) 6 Fr was used to engage left coronary ostium. Runthrough Floppy was wired down LCx. Mid-distal LCx was prepared with Pantera Pro (Biotronik, Germany) 2.5 x 15 mm and DCB Pantera Lux (Biotronik ,Germany) 3.0 x 15 mm was deployed. Finally, we wired down LAD with Runthrough Floppy. Mid-distal LAD lesion was prepared with Pantera Pro 2.5 x 15 mm and DCB Pantera Lux 3.0 x 30 mm was deployed. Proximal LAD lesion, which was calcified, was further prepared with Wolverine 2.5 x 10 mm before DCB Pantera Lux 3.5 x 30 mm was deployed. Final post-PCI results were acceptable, achieving complete revascularisation for him.

Case Summary
Patient with underlying coronary artery disease and active malignancy, who requires invasive coronary intervention poses many challenging issues in term of high bleeding risk, optimal duration and regimes of anti-platelets as well as type of coronary device/strategy chosen for PCI. These group of patient populations are usually excluded from clinical trials. Thus, shared decision making with a multi-disciplinary team approach should be done when assessing the role of invasive coronary intervention for cardiac optimisation in patients with active malignancy who require non-deferrable major tumor resection/chemotherapy/radiotherapy as well as the optimal approach to reduce post-PCI complication.