Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251004_001
Very Elderly Patient, Very Difficult Ostial RCA Lesion (Tips and Tricks for a Quick PCI With Minimal Complications)
By Surenthiran Ramanathan, Chee Kent Er, Chay Shien, Richard Long, Kamaraj Selvaraj, Asri Ranga Abdullah Ramaiah
Presenter
Surenthiran Ramanathan
Authors
Surenthiran Ramanathan1, Chee Kent Er1, Chay Shien, Richard Long2, Kamaraj Selvaraj1, Asri Ranga Abdullah Ramaiah1
Affiliation
Hospital Sultan Idris Shah, Serdang, Malaysia1, Hospital Sultan Idris Shah, Malaysia2
View Study Report
CASE20251004_001
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Very Elderly Patient, Very Difficult Ostial RCA Lesion (Tips and Tricks for a Quick PCI With Minimal Complications)
Surenthiran Ramanathan1, Chee Kent Er1, Chay Shien, Richard Long2, Kamaraj Selvaraj1, Asri Ranga Abdullah Ramaiah1
Hospital Sultan Idris Shah, Serdang, Malaysia1, Hospital Sultan Idris Shah, Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
Patient is very elderly, 86yo, ADL independent. He has Ischaemic Heart Disease - with history of 3VD ( stenting performed 14years ago last ). Co-morbidities include: T2DM, Hypertension, CKD 3a ( related to primary co-morbidities ). He had a recent fall, with no evidence of myocardial infarction. This brought him back to our attention to assess his Coronary status for new evidence of stenosis, arrhythmia or compromised cardiac function.
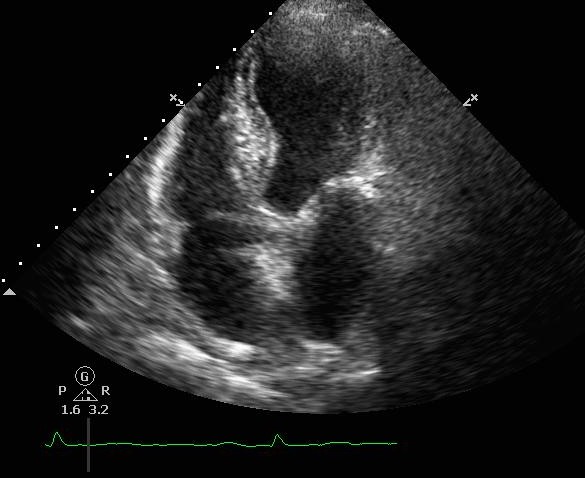
 Echo hypokinesia.mp4
Echo hypokinesia.mp4
Relevant Test Results Prior to Catheterization
ECG showed sinus rhythm. 24hours ECG ( Holter ) showed ectopics < 1% , pause < 2secs [not significant].Echo showed EF 45-50% with hypokinesia (as shown above) – no thrombus or severe aortic stenosis. Creatinine was ~130umol/L ( not markedly raised).Ad hoc Coronary Angiography was performed:LM <30% stenosesLAD Prox 70-80%LCx ISR (Prox-Mid) 80-90%RCA ISR (Pros) 80% , DominantPCI to LCx ISR – DEB 2.75/20mm , PCI to LAD (ostium-mid) – DES 2.75/33mm + 3.5/13mm
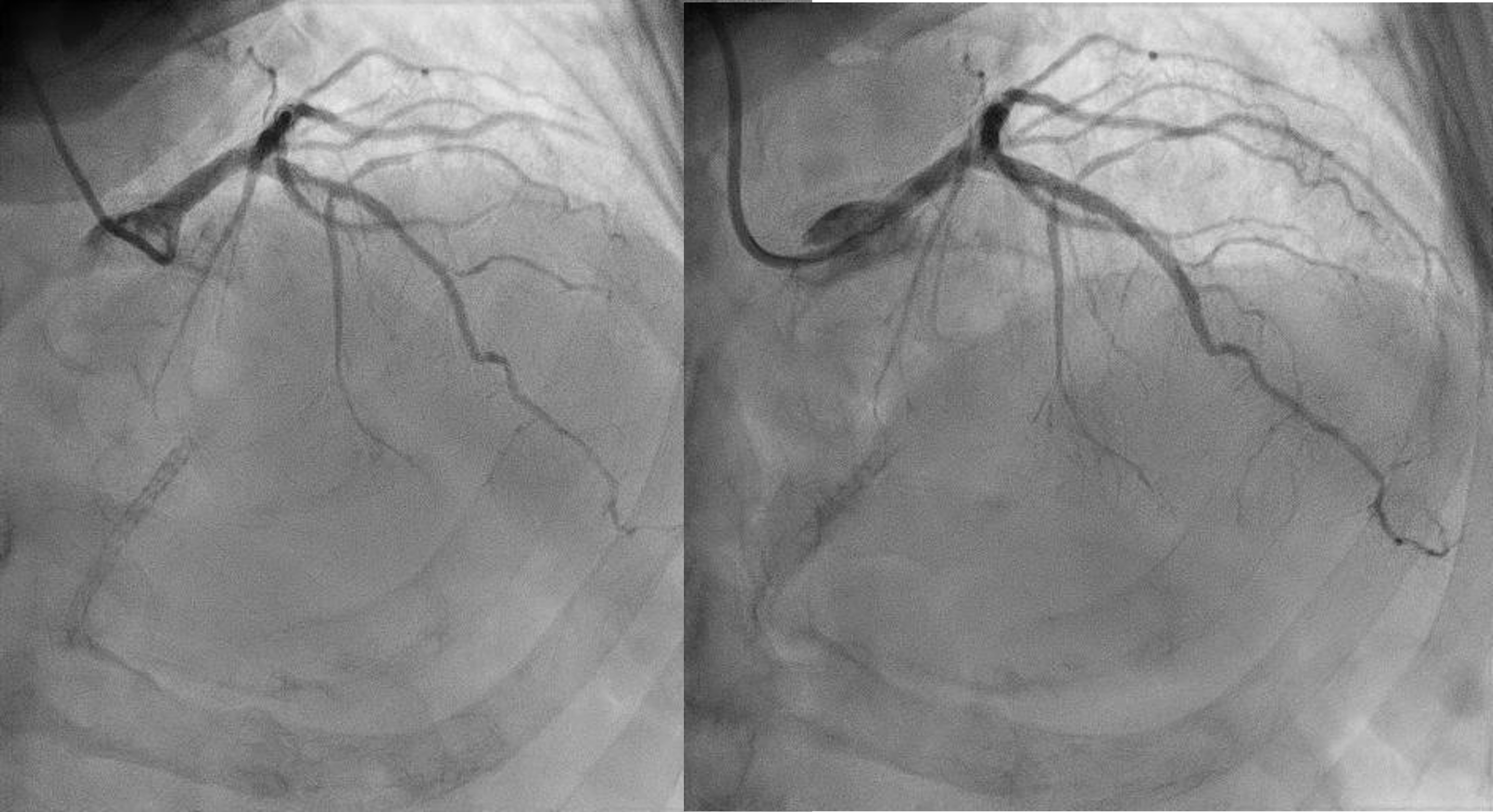
Diagnostic Angio Lt system.mp4
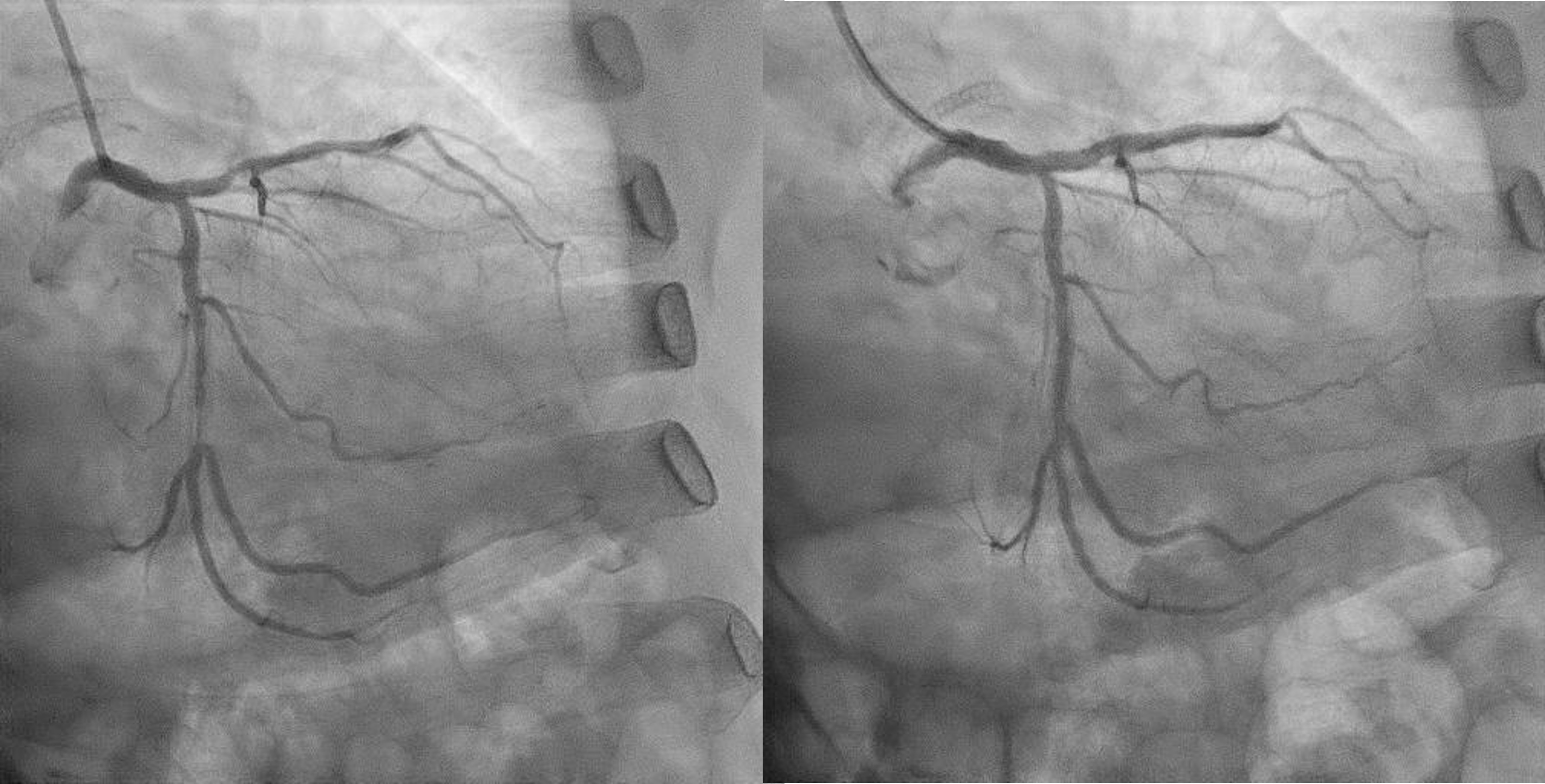
PostPCI LAD.wmv
Post PCI Lcx.wmv
Relevant Catheterization Findings
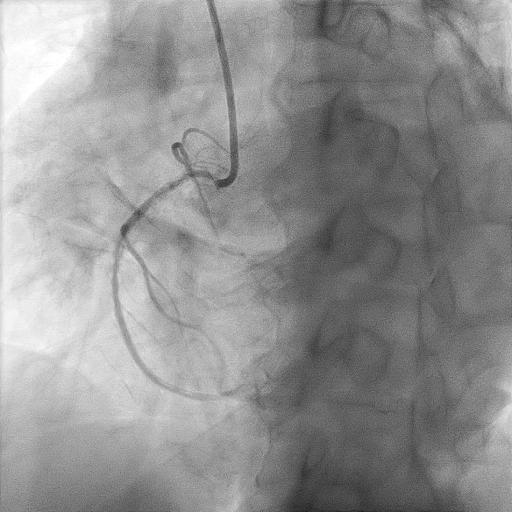
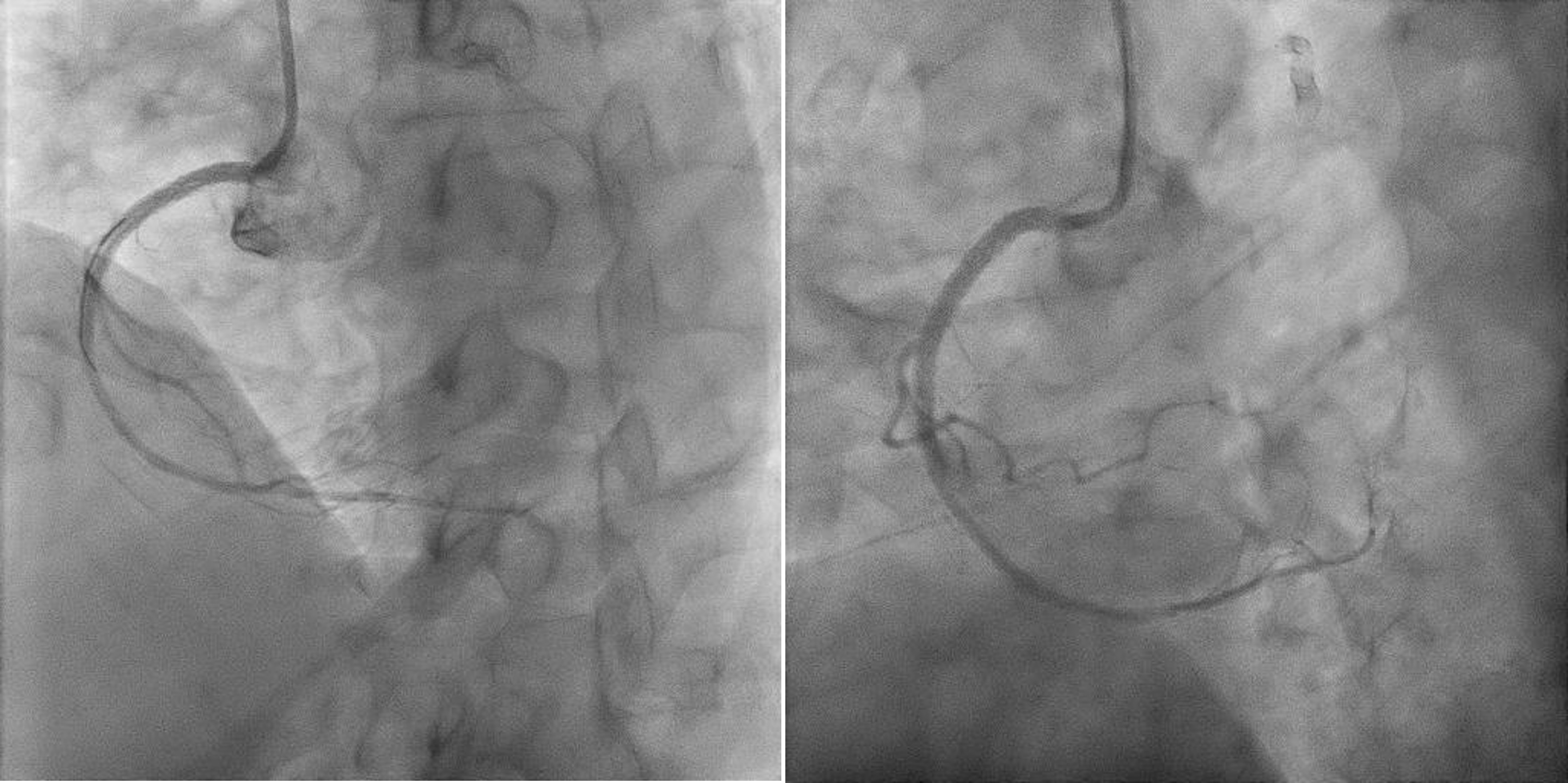
Now for staged PCI to RCA. Attempted engagement with a JR 3.5 6Fr via RRA.Challenges anticipated:1 subclavian tortuosity, noted from past angiography – needing gentle manipulation, avoid femoral access2 poor engagement due to ostium disease3 wiring from outside ( ‘air-mail’)Lesions are calcifed, diffuse, proximal(ostium RCA) and distal to stented segment - stent not covering ostium.Plan is to IVUS, prepare new lesions, prepare ISR segments then either hybrid DES/DEB or new DES all the way.
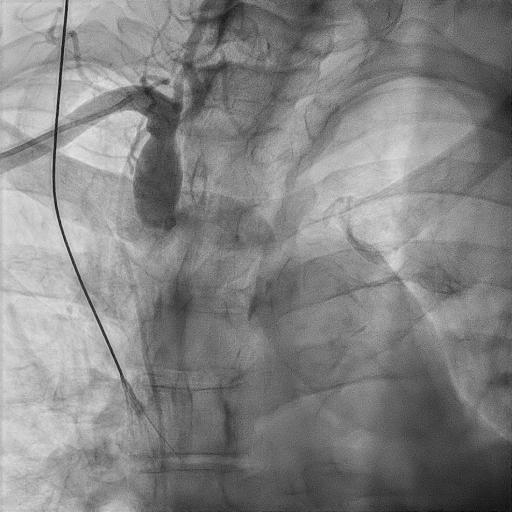
Subclavian tortuosity.jpg
Subclavian tortuosity.wmv
Diagnostic RCA.mp4
Airmail wire into RCA.wmv
Interventional Management
Procedural Step
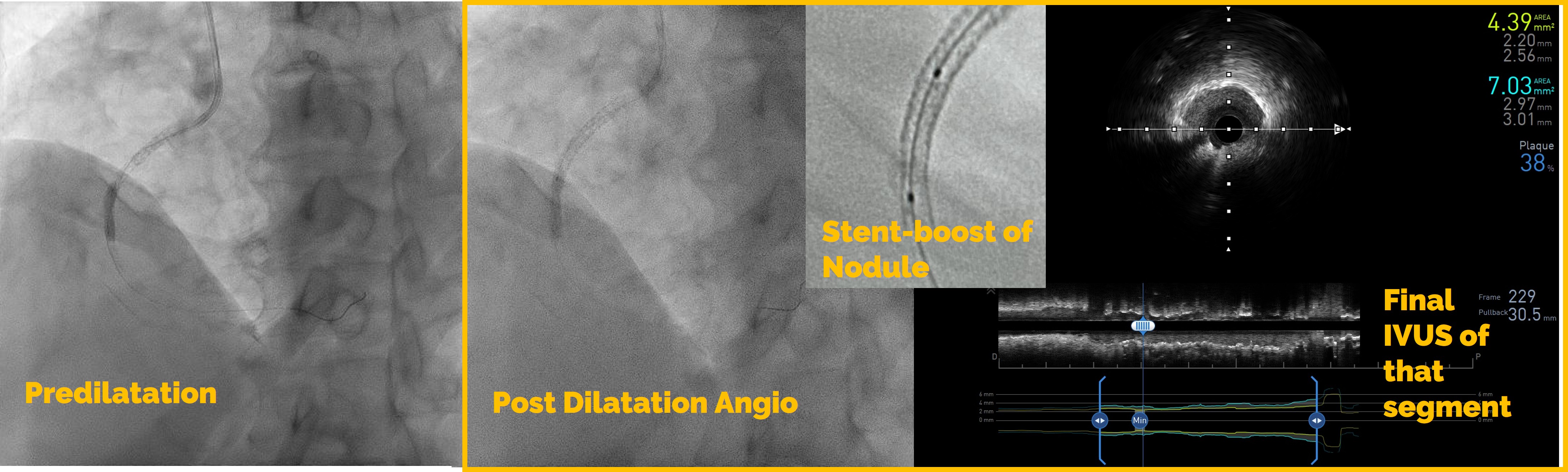
1 Initial predilatation with NC 3.0 > IVUS > Scoring 3.5 up till ostiumIVUS findings showed fibrocalcific+ nodular calcific plaques within and beyond stentRCA sizing was between 3.0mm till 4.0mm proximallyStent was long standing - likely adequately sized Smallest lumen was 1.83mm2 2 Just prior stenting another IVUS performedSmallest lumen (same as previous) improved > 4.0mm23 Long DES 3.0/48mm deployed > Postdilated with NC 3.5 then NC 4.04 Final IVUS performed, stents well opposed, ostium covered adequately but smalles lumen was 4.39mm2
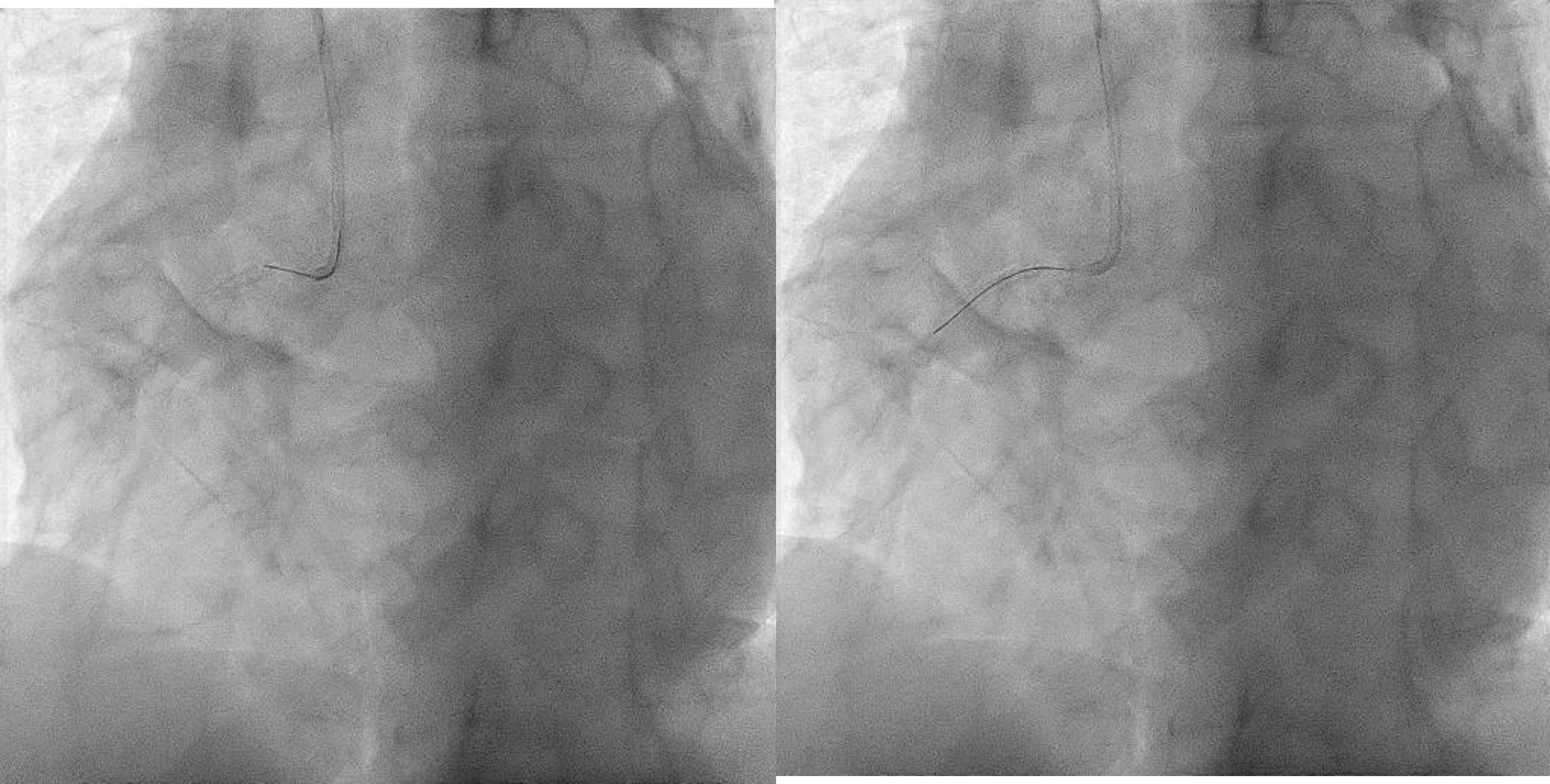
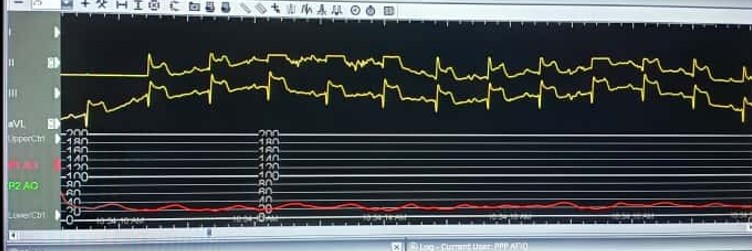
Challenges:1 During PCI, ostium lesion causes BP dampening + ST elevations - catheter kept outside ostium during entire PCI2 Wiring was done from outside - 'air mail'ed into the RCA3 Long stent needed delivering - used 'buddy wire' technique to deliver this4 Findings exact ostium was tough - 'buddy wire' converted to 'sepal wire' for better outcome5 During postdilatation, the 'stubborn' nodule at the distal part of stent, was difficult to prepareEven after stenting, IVUS improvement only. Stent boost was used to delineate the calcific nodular area.
Entire procedure was 36minutes with contrast ~ 150mls. Patient was discharged well with no haemodynamic compromise.
Buddy wire technique to deliver Long Sten.wmv
Nailing the RCA ostium.wmv
Final RCA Angio.wmv
Challenges:1 During PCI, ostium lesion causes BP dampening + ST elevations - catheter kept outside ostium during entire PCI2 Wiring was done from outside - 'air mail'ed into the RCA3 Long stent needed delivering - used 'buddy wire' technique to deliver this4 Findings exact ostium was tough - 'buddy wire' converted to 'sepal wire' for better outcome5 During postdilatation, the 'stubborn' nodule at the distal part of stent, was difficult to prepareEven after stenting, IVUS improvement only. Stent boost was used to delineate the calcific nodular area.
Entire procedure was 36minutes with contrast ~ 150mls. Patient was discharged well with no haemodynamic compromise.
Case Summary
As titled, this case highlighted:1 A very elderly patient - who he can deteriorate and if so, will be difficult to recover2 Ostium RCA lesion which made engagement impossible and also fatal if not carefulWe employed many tips and tricks with the sole purpose of completing the PCI in the quickest yet safest option possible - as illustrated above. In any case, if anything unfavourable occurred, we must be prepared to convert to femoral access, get help, use more devices and standby haemodynamic support.The last part, when we accepted the slightly undersized segment, clearly showed nothing can be perfect and 'chasing' endless results, may lead to the PCI not being completed successfully.