Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251001_001
A Tale of Lost and Left-Behind Stent
By Aditi Ajit Newaskar, Krishna Prasad Nevali
Presenter
Krishna Prasad Nevali
Authors
Aditi Ajit Newaskar1, Krishna Prasad Nevali2
Affiliation
AIIMS Mangalagiri, India1, NRI Medical College, India2
View Study Report
CASE20251001_001
Coronary - Complication Management
A Tale of Lost and Left-Behind Stent
Aditi Ajit Newaskar1, Krishna Prasad Nevali2
AIIMS Mangalagiri, India1, NRI Medical College, India2
Clinical Information
Relevant Clinical History and Physical Exam
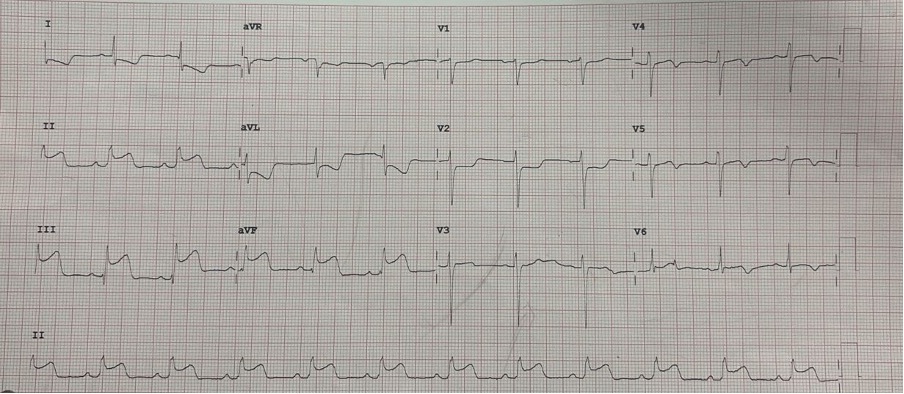
A 67 year old male presented to emergency room with chest pain of 1 hour duration. Chest pain was central radiating to left arm and is associated with nausea, vomiting and diaphoresis.Electrocardiogram showed ST elevation in lead 2, 3, aVF sugesting inferior wall myocardial infarction (Figure 1). Echocardiogram showed no mechanical complications and an ejection fraction of 50 % with inferior wall hypokinesia. He was treated with dual antiplatelets, statin and low moilecular weight heparin
Relevant Test Results Prior to Catheterization
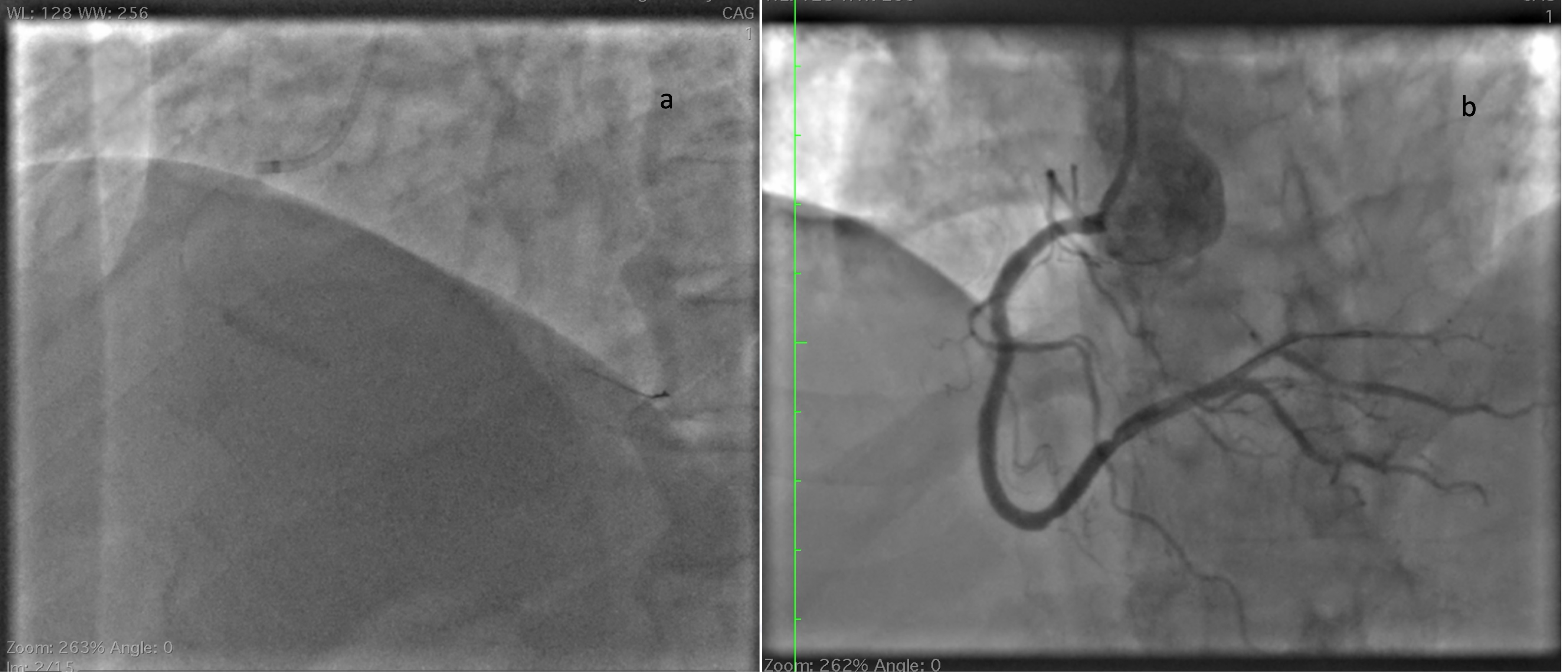
He was immediately shifted to catheterization laboratory and angiogram showed mild plaque in left anterior descending artery (Figure 2)(Video 1) and significant stenosis In distal right coronary artery with additional mild plaque proximally (Figure 3) (video 2).
Relevant Catheterization Findings
He was immediately shifted to catheterization laboratory and angiogram showed mild plaque in left anterior descending artery (Figure 2)(Video 1) and significant stenosis In distal right coronary artery with additional mild plaque proximally (Figure 3) (video 2).

 video 1.mov
video 1.mov
video 2.mov
Interventional Management
Procedural Step
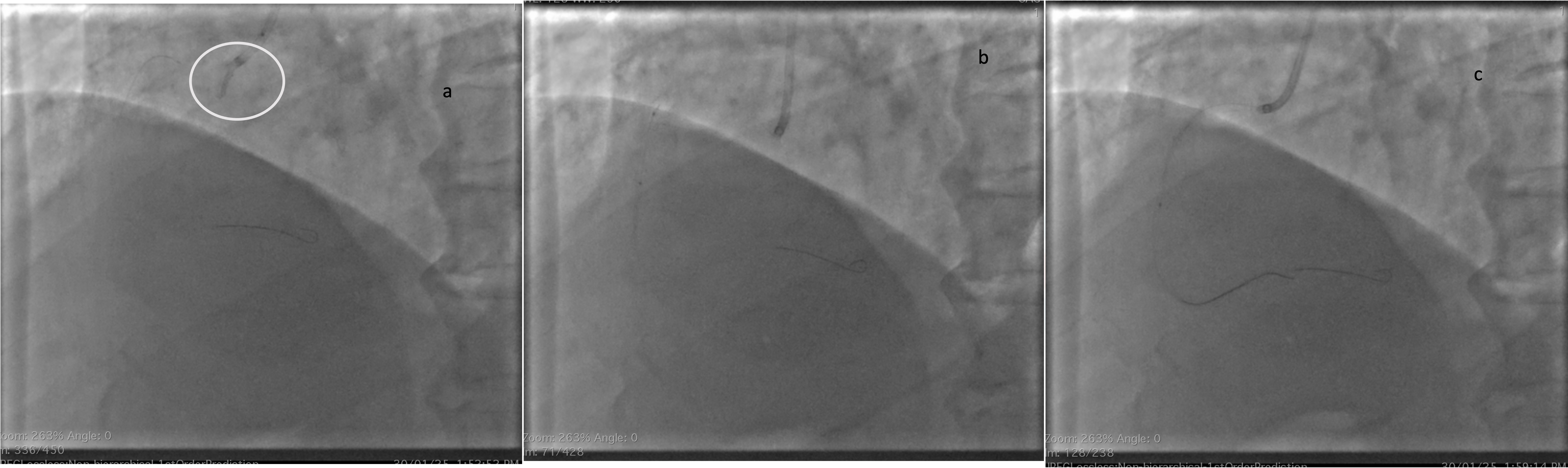
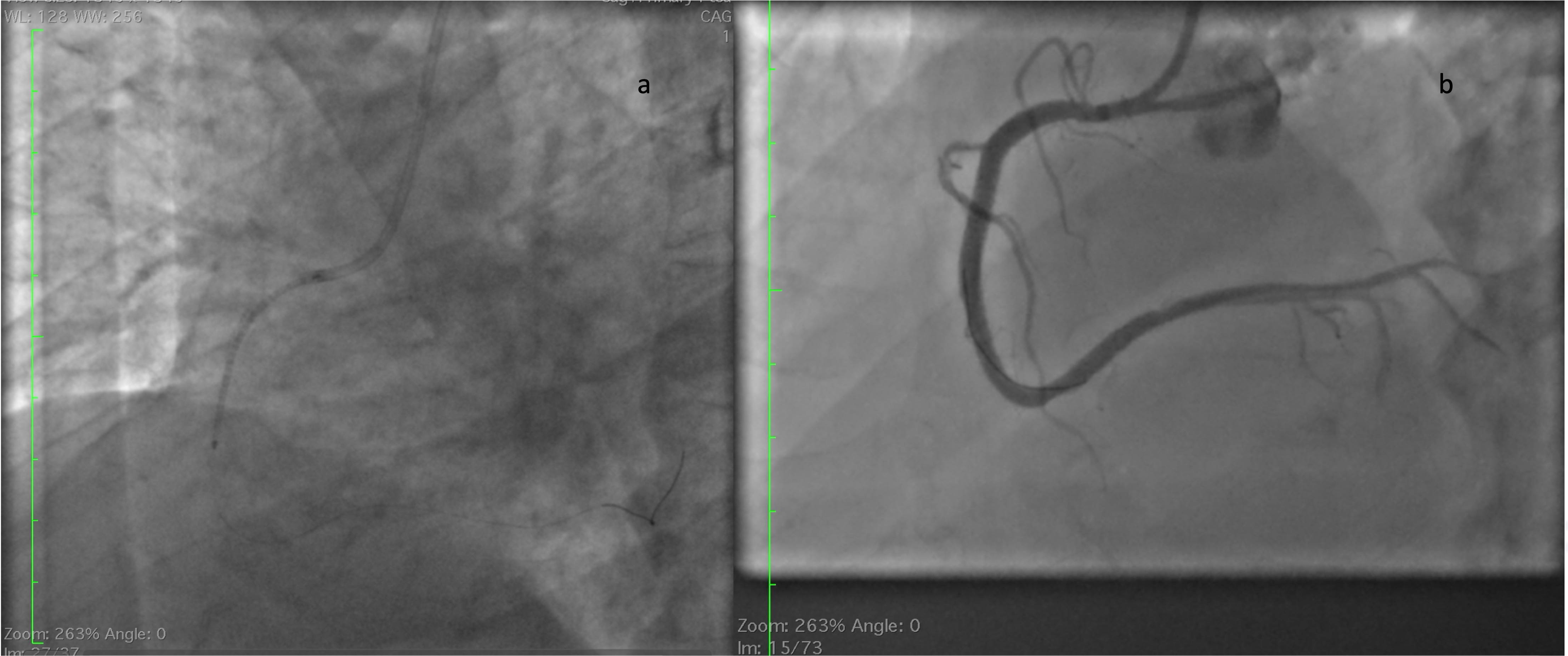
Immediately a 6 French JR 3.5 catheter was taken and right coronary artery ostium was engaged. Then a work horse wire was parked distally in posterolateral vein branch. Then a 2.75 x 23 mm Drug eluting stent was deployed across the lesion (Figure 4a). After deployment angiogram showed haziness at the distal edge of the stent. Nitroglycerine, nicorandil and tirofiban injections were given and check angiogram showed no improvement in the distal edge haziness (figure 4b). In view of possible dissection it was decided to cover the distal edge with one more DES. While passing the second DES due to poor catheter support manipulation led to degloving of the stent from balloon (figure 5a).
videoo 3.mov
video 4.mov
video 5.mov
Case Summary
Stent degloving is an avoidable complication. If not tackled can lead to CVA due to embolization to cerebral vessels. Guide support is extremely important even in normal looking RCA. Use of better supporting guides like AL 1 or AL 0.75 can prevent these complications. All techniques of stent degloving should be known to manage such complications.