Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20250905_002
Safe Passage: Carotid Protection During Balloon Mitral Valvotomy in Rheumatic Mitral Stenosis With Left Atrial Appendage Clot
By Rupendra Saha Saha, Bhanu Duggal
Presenter
Rupendra Saha Saha
Authors
Rupendra Saha Saha1, Bhanu Duggal1
Affiliation
Aiims Rishikesh , India1
View Study Report
CASE20250905_002
Structural - Other Structural Interventions
Safe Passage: Carotid Protection During Balloon Mitral Valvotomy in Rheumatic Mitral Stenosis With Left Atrial Appendage Clot
Rupendra Saha Saha1, Bhanu Duggal1
Aiims Rishikesh , India1
Clinical Information
Relevant Clinical History and Physical Exam
A 54-year-old frail woman with long-standing rheumatic heart disease presented with worsening dyspnoea, abdominal distension, jaundice, and pedal oedema. She was in atrial fibrillation with irregularly irregular pulse, variable S1, and a mid-diastolic murmur at the apex. She had signs of right heart failure with tense ascites and hepatomegaly.
Relevant Test Results Prior to Catheterization
ECG: atrial fibrillation with rapid ventricular rate.
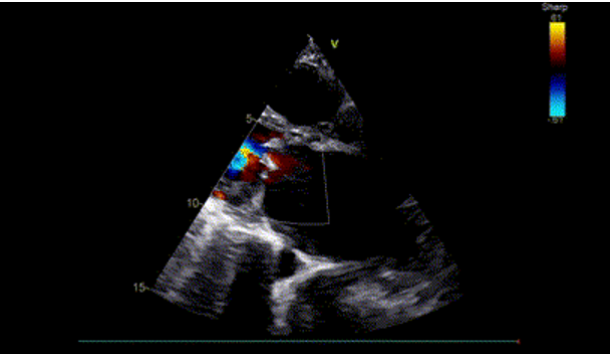
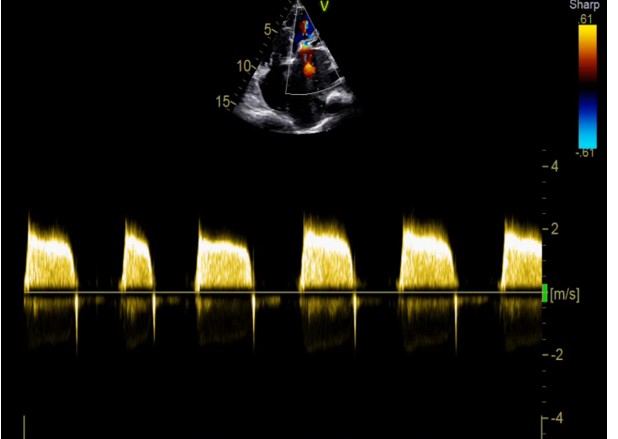
TTE: severe rheumatic mitral stenosis (MVA <1 cm²), dilated LA, severe pulmonary hypertension (TR gradient >70 mmHg).
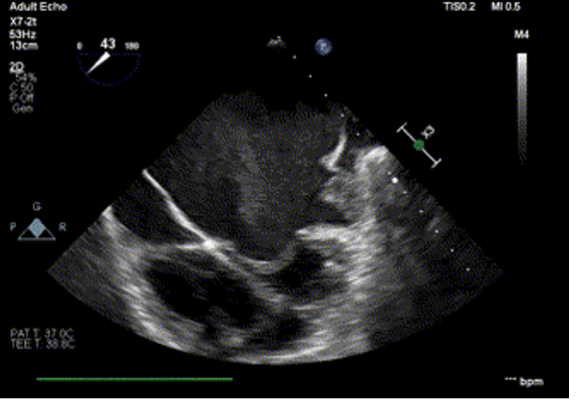
TEE: Type IB left atrial appendage thrombus, thin interatrial septum, no significant mitral regurgitation.
Laboratory: elevated bilirubin, mild deranged INR.
TTE: severe rheumatic mitral stenosis (MVA <1 cm²), dilated LA, severe pulmonary hypertension (TR gradient >70 mmHg).
TEE: Type IB left atrial appendage thrombus, thin interatrial septum, no significant mitral regurgitation.
Laboratory: elevated bilirubin, mild deranged INR.
Relevant Catheterization Findings
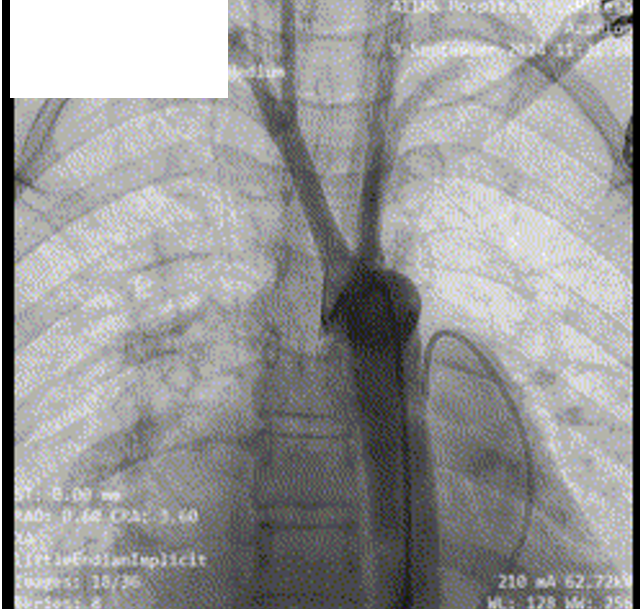
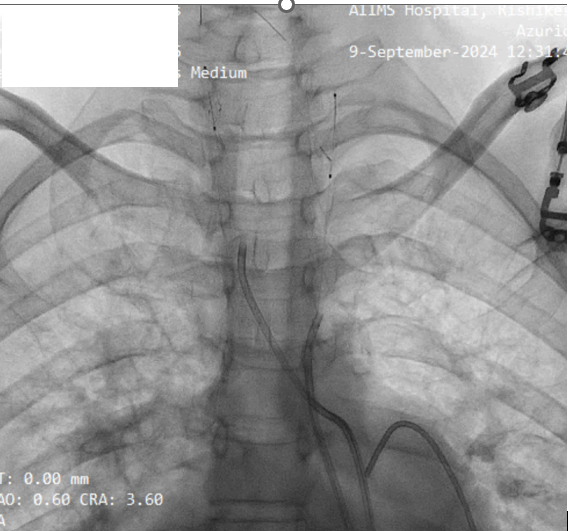
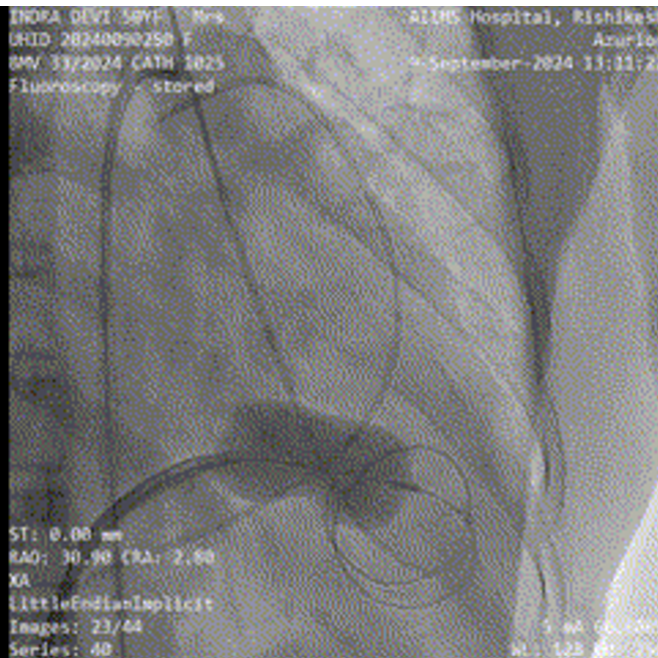
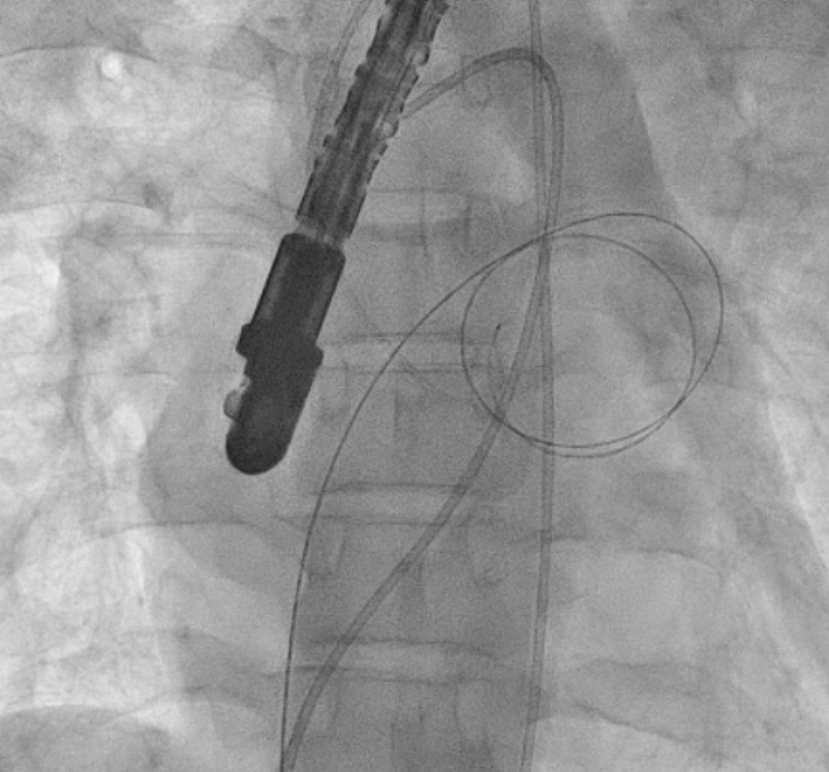
Given prohibitive surgical risk, high-risk BMV was attempted. Bilateral carotid angiography was performed and SpiderFx embolic protection devices (Medtronic, USA) deployed. Under TEE guidance, transseptal puncture was done, and an Inoue balloon (Toray, Japan) was advanced across the mitral valve. Sequential dilatations reduced the mean gradient with no embolic debris in filters. The patient improved hemodynamically and was discharged in stable condition.
Interventional Management
Procedural Step
The patient was deemed prohibitive risk for surgical mitral valve replacement with clot extraction, so a high-risk percutaneous approach was planned. Bilateral carotid angiography was performed, and 5 mm SpiderFx embolic protection devices (Medtronic, Minneapolis, MN, USA) were deployed to minimize embolic risk. Transseptal puncture was guided by transesophageal echocardiography because of a thin interatrial septum. An Inoue balloon catheter (Toray, Tokyo, Japan) was advanced across the mitral valve, and sequential graded dilatations were performed under fluoroscopy. Mean transmitral gradient fell markedly, with corresponding fall in pulmonary artery pressure. The embolic filters were retrieved without visible debris. The procedure was uneventful, with no neurological events. The patient was extubated on table, remained hemodynamically stable, and reported significant symptomatic improvement. She was discharged in NYHA class II and, at follow-up, was able to resume routine activities with sustained benefit.
Case Summary
Emergency BMV remains a lifesaving therapy in advanced rheumatic MS, especially in LMICs. The presence of LAA clot is usually a contraindication due to risk of embolic stroke. This case demonstrates the feasibility of performing BMV with simultaneous bilateral carotid protection, ensuring neurological safety. Wider adoption of such innovative approaches, along with better RHD awareness, structured referral, and availability of essential devices, can improve outcomes in neglected populations where surgical options are limited.