Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20250815_001
A Challenging Case Report of Percutaneous Coronary Intervention (PCI) of Complex Chronic Total Occlusion (CTO) Left Anterior Descending Artery (LAD) via Right Distal Radial Access With 5 Fr Ikari
By Sajja Jangjit, Wittawat Wattanasiriporn
Presenter
Sajja Jangjit
Authors
Sajja Jangjit1, Wittawat Wattanasiriporn1
Affiliation
College of Medicine, Rangsit University, Division of Cardiology, Rajavithi Hospital, Bangkok, Thailand1
View Study Report
CASE20250815_001
Coronary - Complex PCI - CTO
A Challenging Case Report of Percutaneous Coronary Intervention (PCI) of Complex Chronic Total Occlusion (CTO) Left Anterior Descending Artery (LAD) via Right Distal Radial Access With 5 Fr Ikari
Sajja Jangjit1, Wittawat Wattanasiriporn1
College of Medicine, Rangsit University, Division of Cardiology, Rajavithi Hospital, Bangkok, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
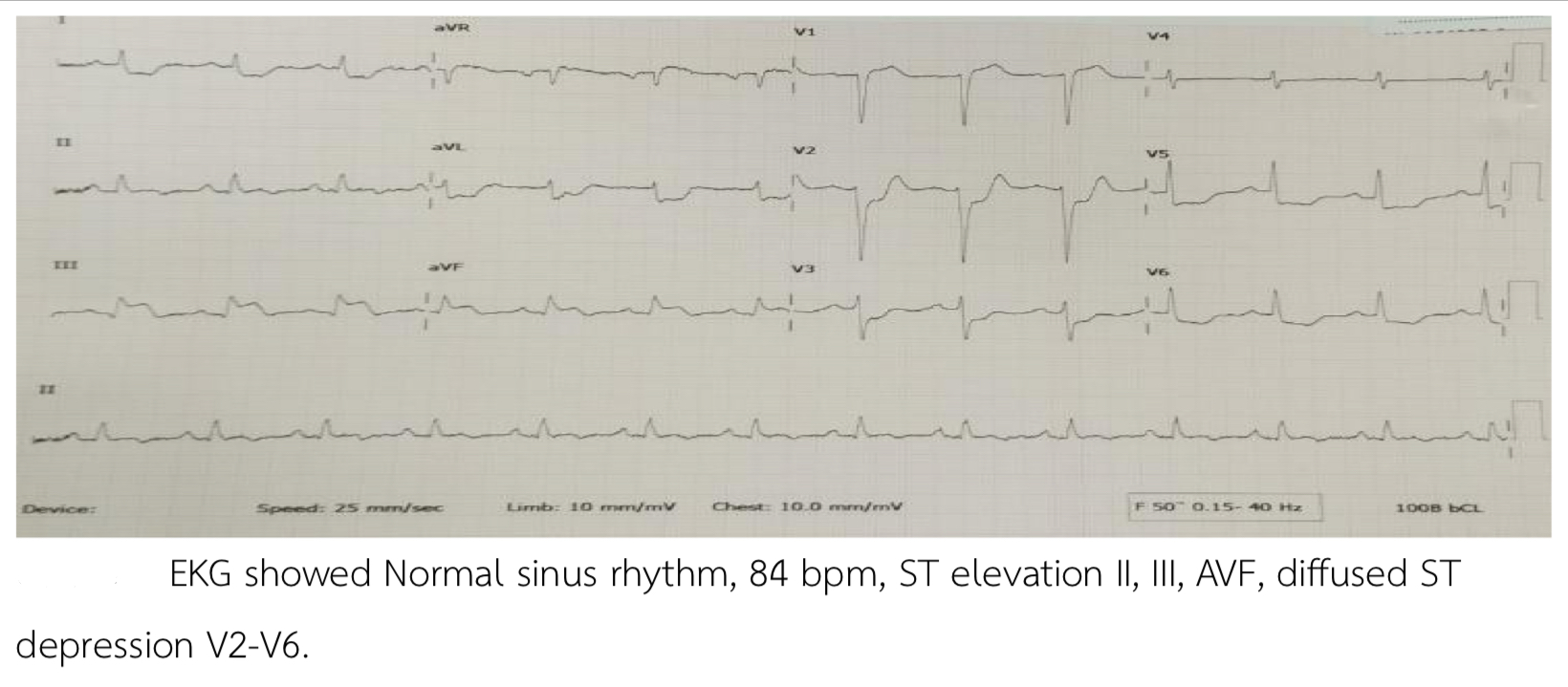
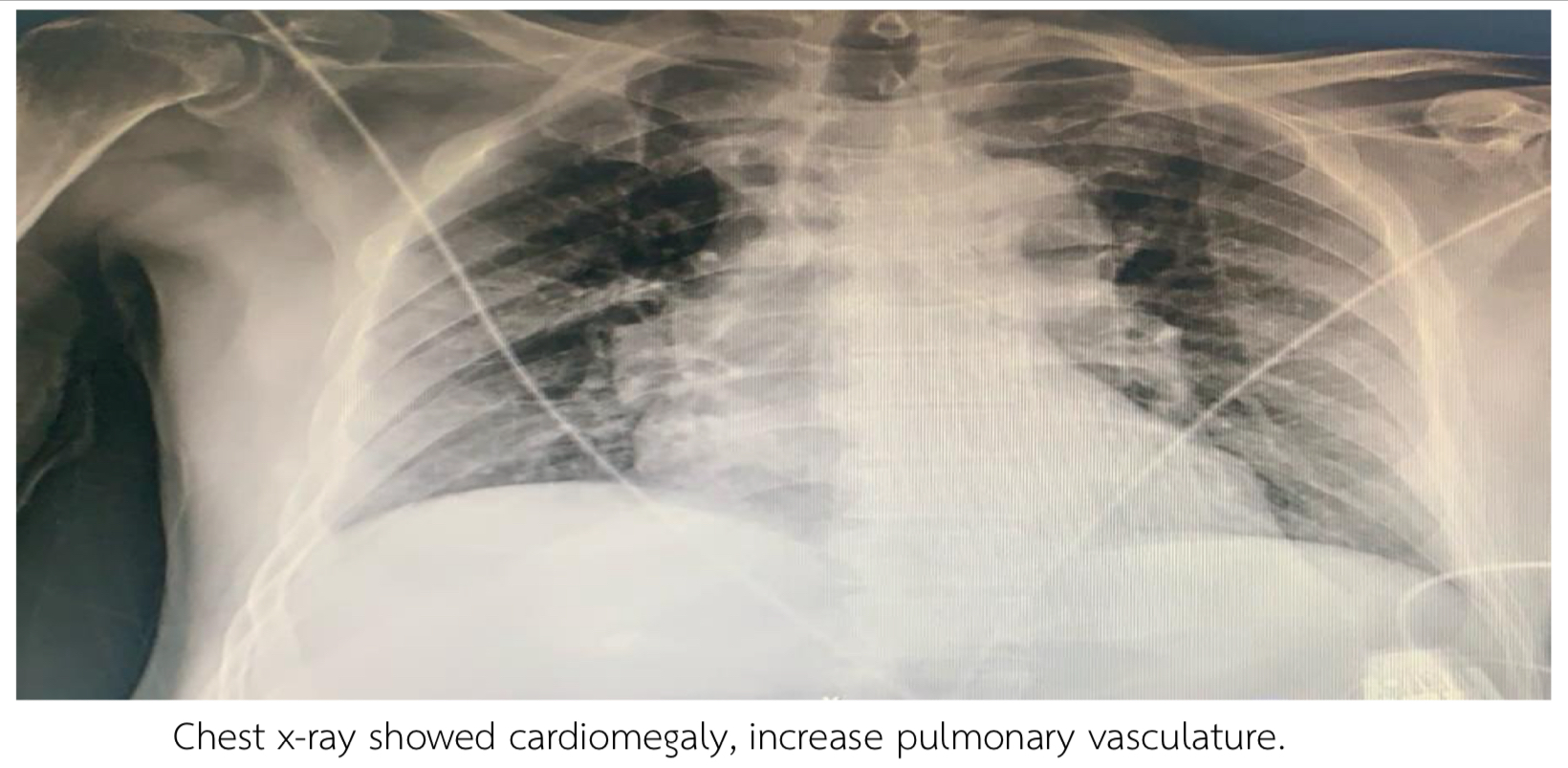
Thai male 69 years, Risk HT, DLP presented with chest pain 2 hours prior to admission. BP 104/62 mmHg HR 76 bpm. Heart regular, fine crepitation both lower lungs. EKG showed NSR, 84 bpm, STE II, III, AVF, diffused STD V2-V6. Echo showed LVEF 42%, Global wall Hypokinesia, no significant VHD. Troponin T was positive 10,400 pg/ml. Chest x-ray showed cardiomegaly, increase pulmonary vasculature.
Relevant Test Results Prior to Catheterization
EKG showed NSR, 84 bpm, STE II, III, AVF, diffused STD V2-V6. Echo showed LVEF 42%, Global wall Hypokinesia, no significant VHD. Troponin T was positive 10,400 pg/ml. Chest x-ray showed cardiomegaly, increase pulmonary vasculature.
Relevant Catheterization Findings
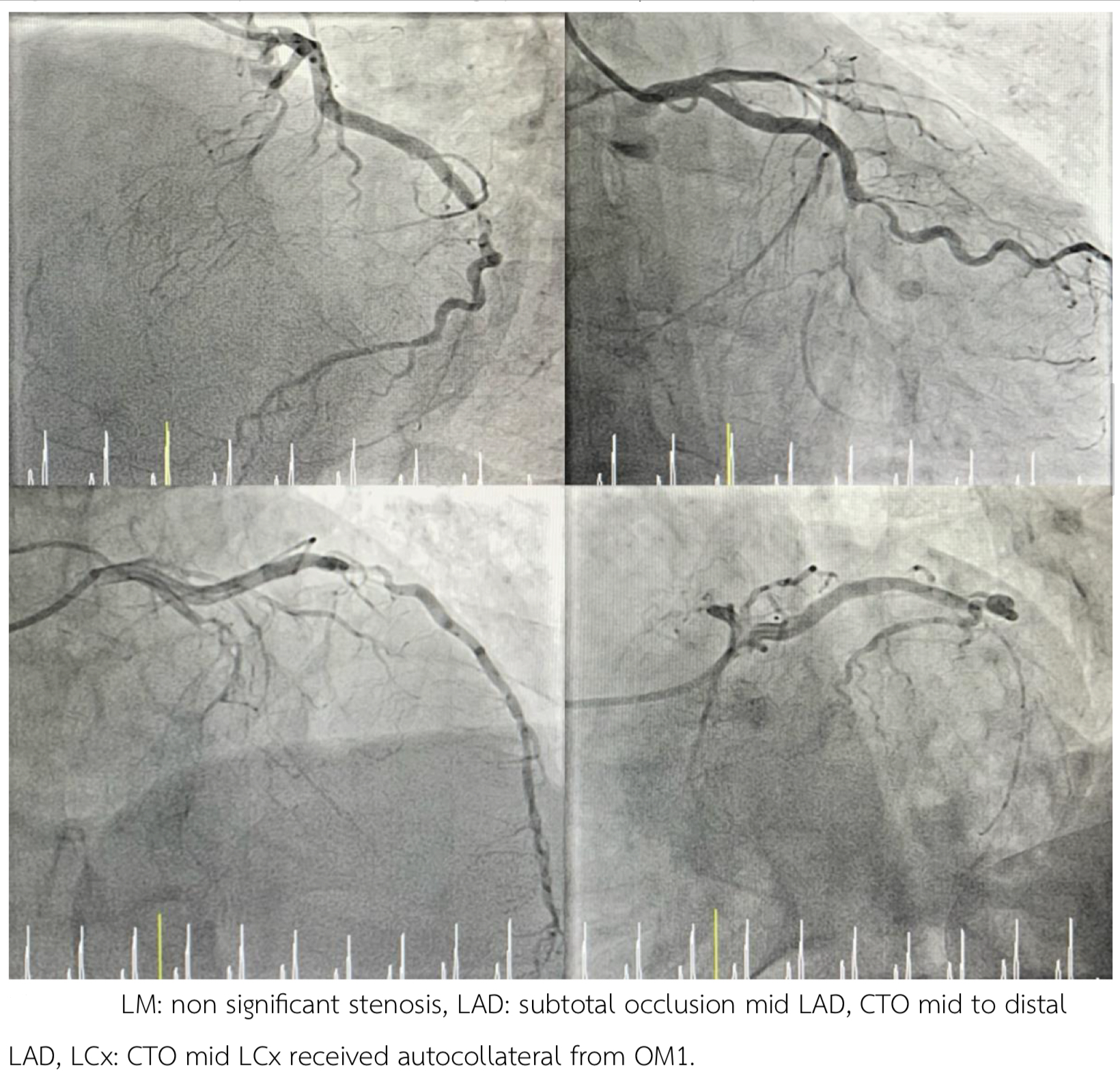
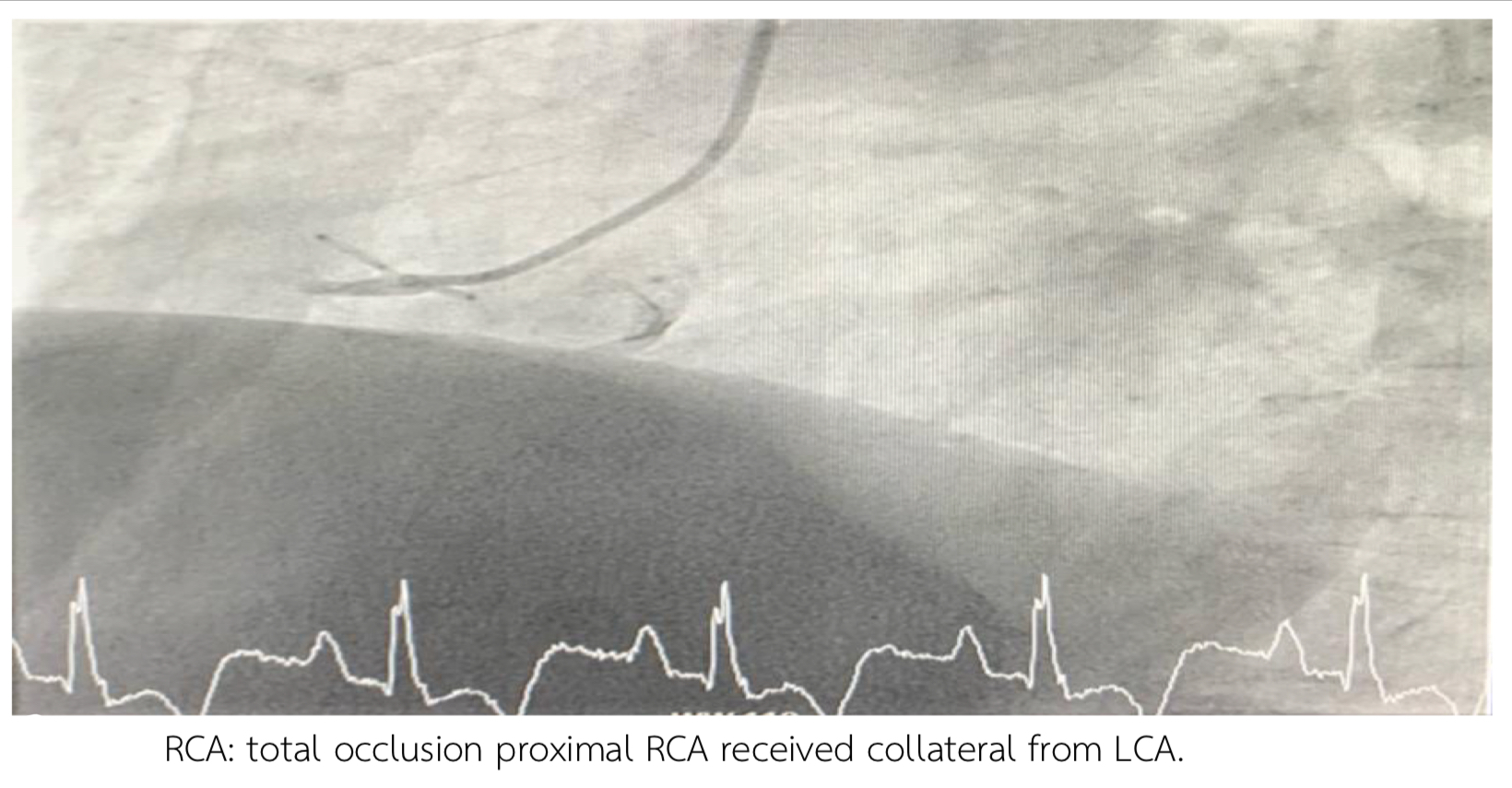
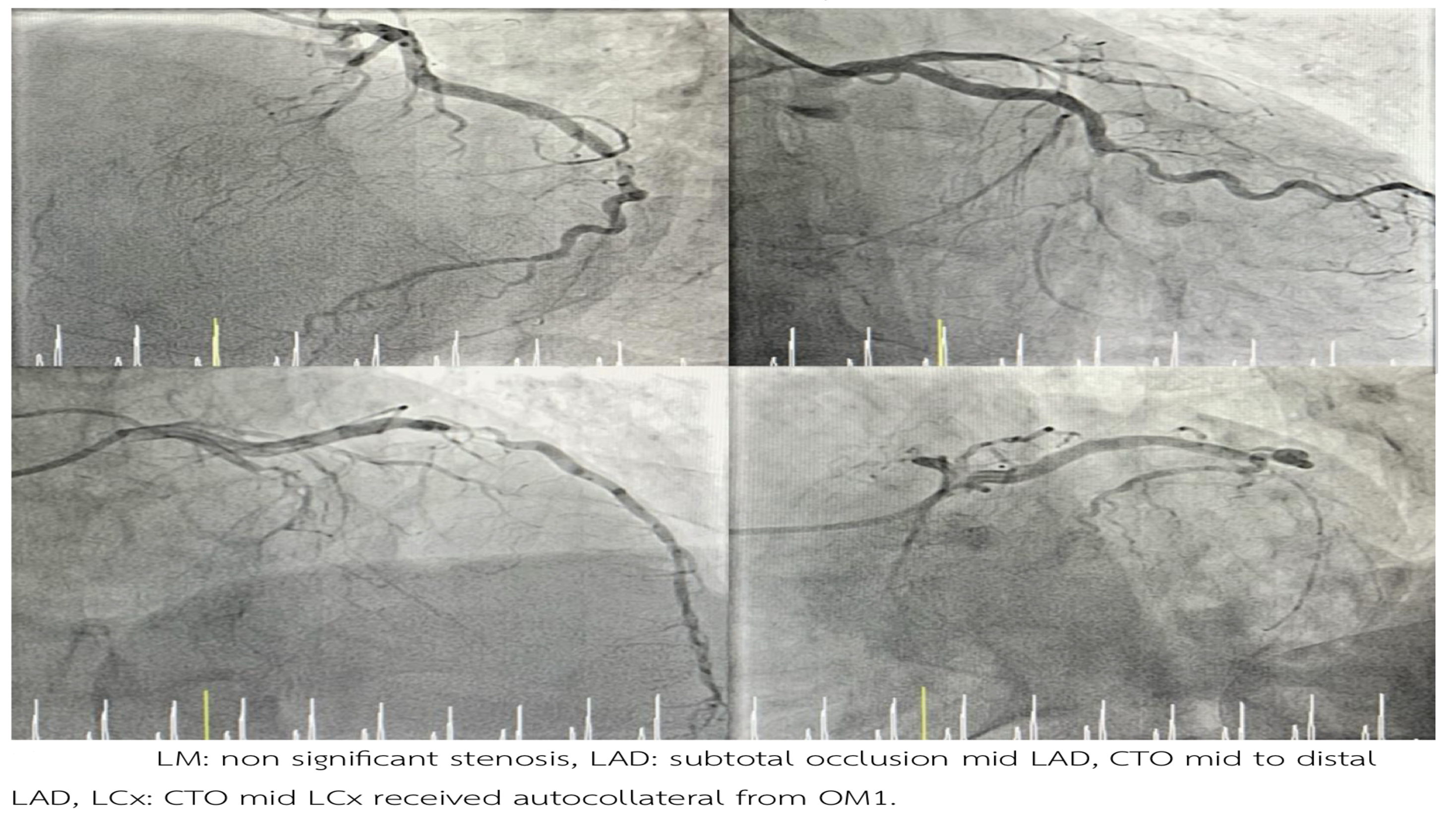
- LM: non significant stenosis
Interventional Management
Procedural Step
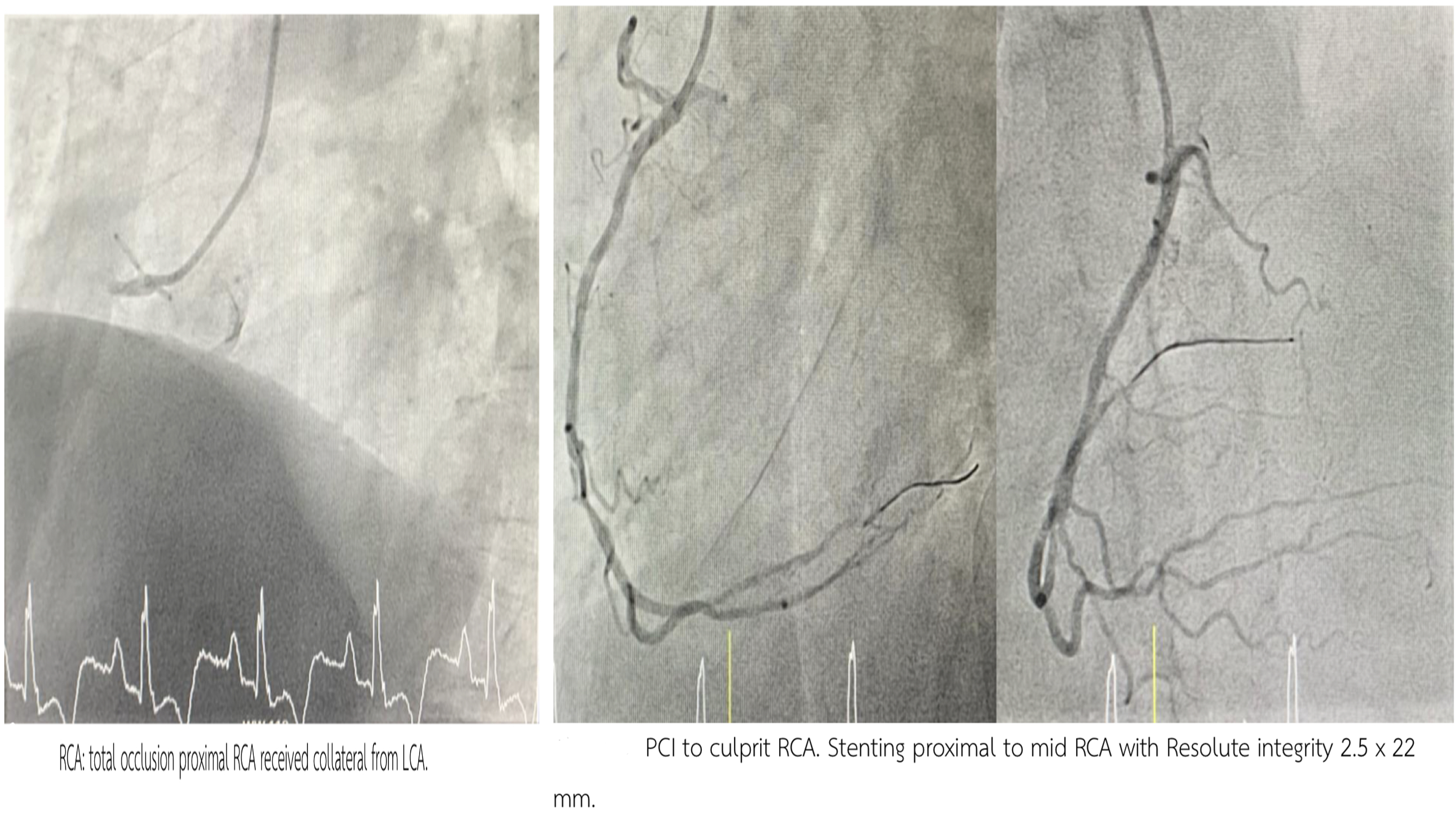
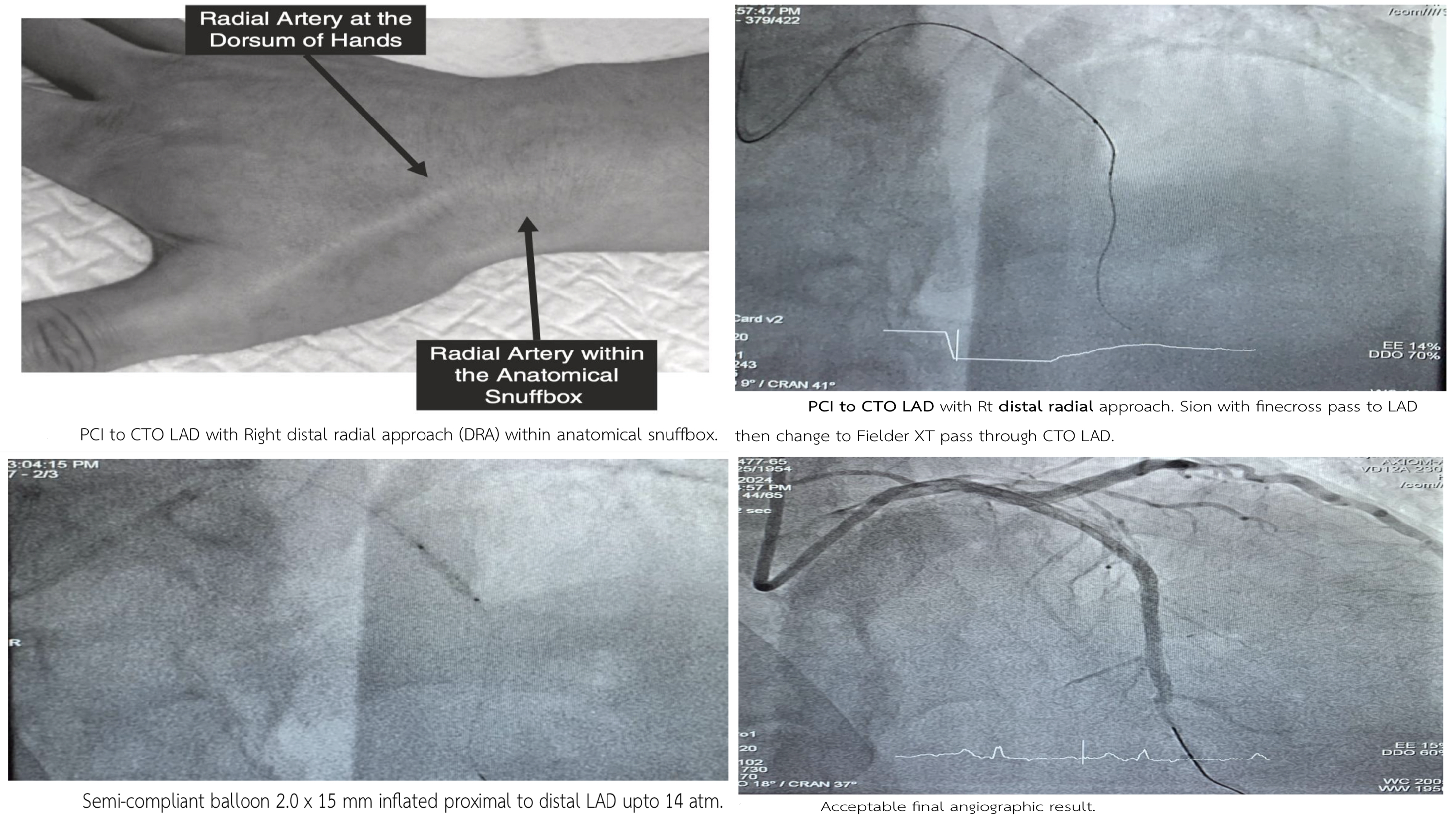
PCI to culprit RCA via Rt radial. The patient still had chest pain then stage PCI to CTO LAD with Rt DRA. Staged PCI to CTO LAD via Rt DRA.
Case Summary
1. DRA is a feasible and safe alterative for complex PCI.