Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20250813_001
Power of Collateral: Survival Patient With Left Main Coronary Artery Total Occlusion
By Saovichet Ly
Presenter
Saovichet Ly
Authors
Saovichet Ly1
Affiliation
Cambodia-China Friendship Preah Kossamak Hospital, Cambodia1
View Study Report
CASE20250813_001
Coronary - ACS/AMI
Power of Collateral: Survival Patient With Left Main Coronary Artery Total Occlusion
Saovichet Ly1
Cambodia-China Friendship Preah Kossamak Hospital, Cambodia1
Clinical Information
Relevant Clinical History and Physical Exam
The patient was a 76-year-old male with past medical history of hypertension. He has had a three months history of exertional chest pain. He was admitted to emergency department for worsening chest pain. His hemodynamic status was stable upon arrival.
Relevant Test Results Prior to Catheterization
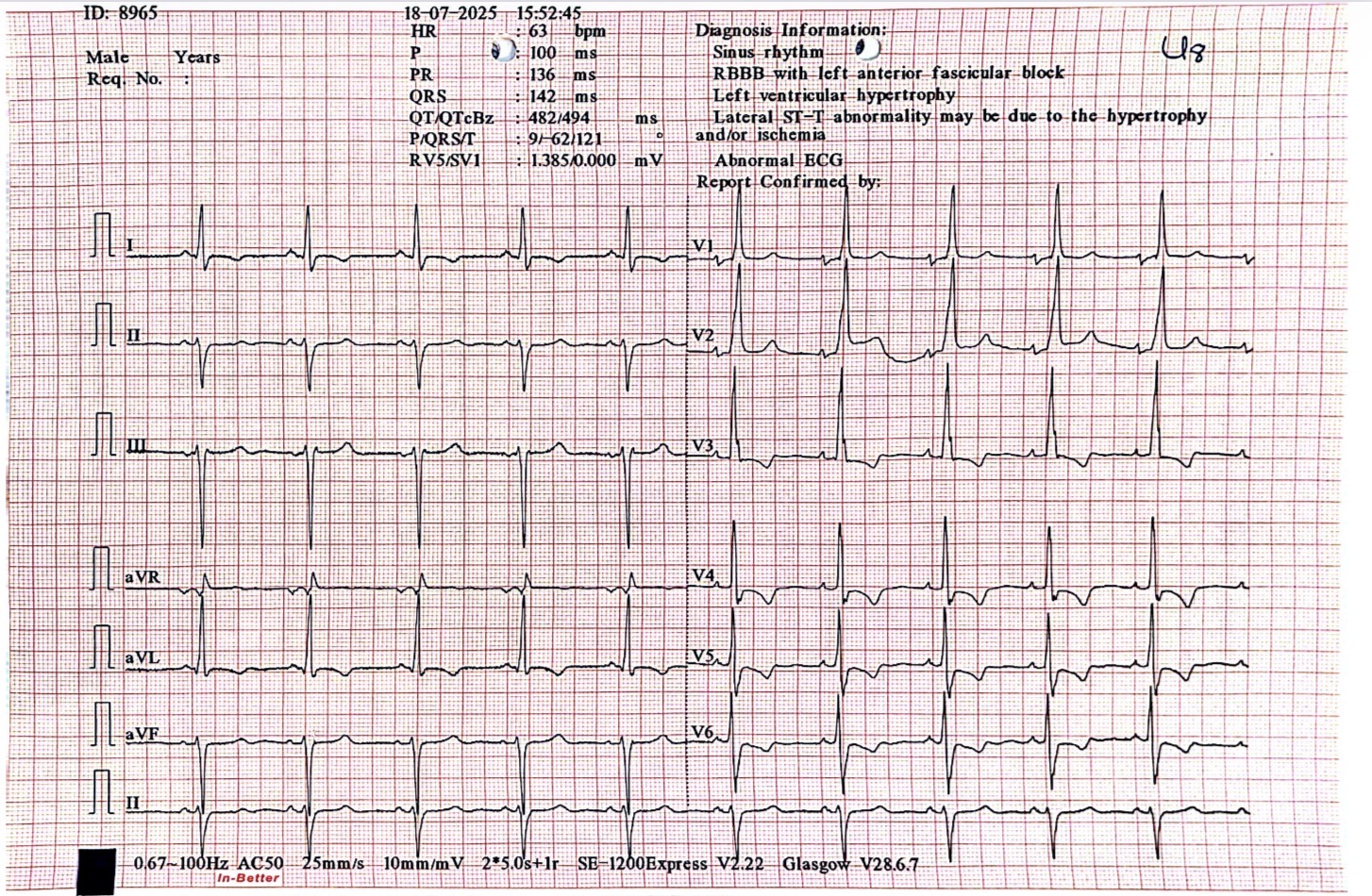
Electrocardiography showed ST-segment depression with T wave inversion at V3-V6, DI, and aVL. Heart ultrasound found hypokinesia of anterior, septal, lateral and apical segment of LV wall with reduced LV systolic function (LVEF 35%), with normal LV filling pressure.Troponin-T was elevated at 0.314 ng/ml. Rest of the laboratory parameters were within normal range.
Relevant Catheterization Findings
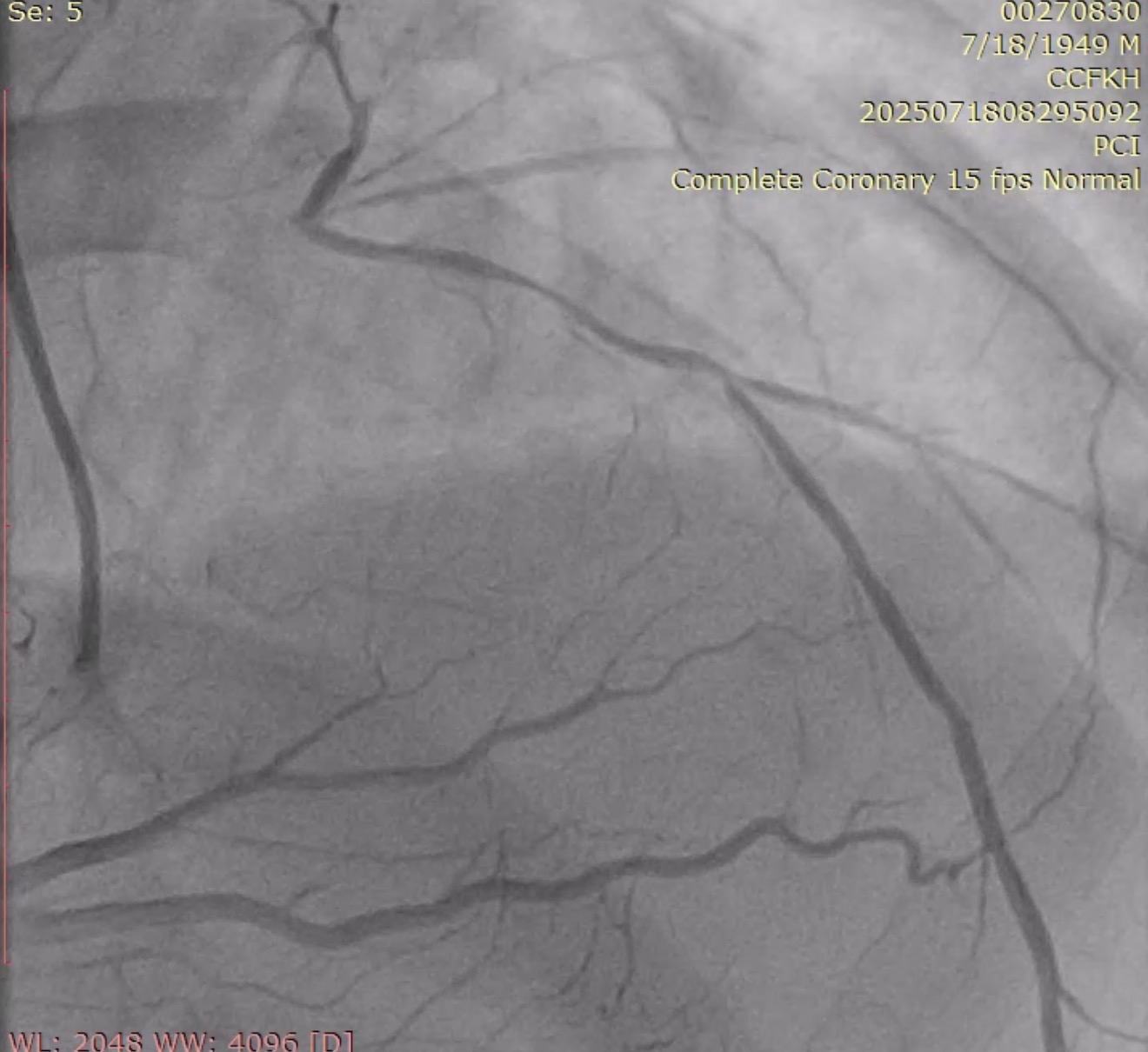
Urgent coronary angiography was performed by using right radial artery approach, which surprisingly showed left main coronary artery (LMCA) total occlusion with TIMI 0 flow. Right coronary artery has no significant stenosis with presence of excellent collaterals flow to the total left coronary system (Rentrop-3).

 CAG1.mov
CAG1.mov
CAG2.mov
CAG3.mov
Interventional Management
Procedural Step
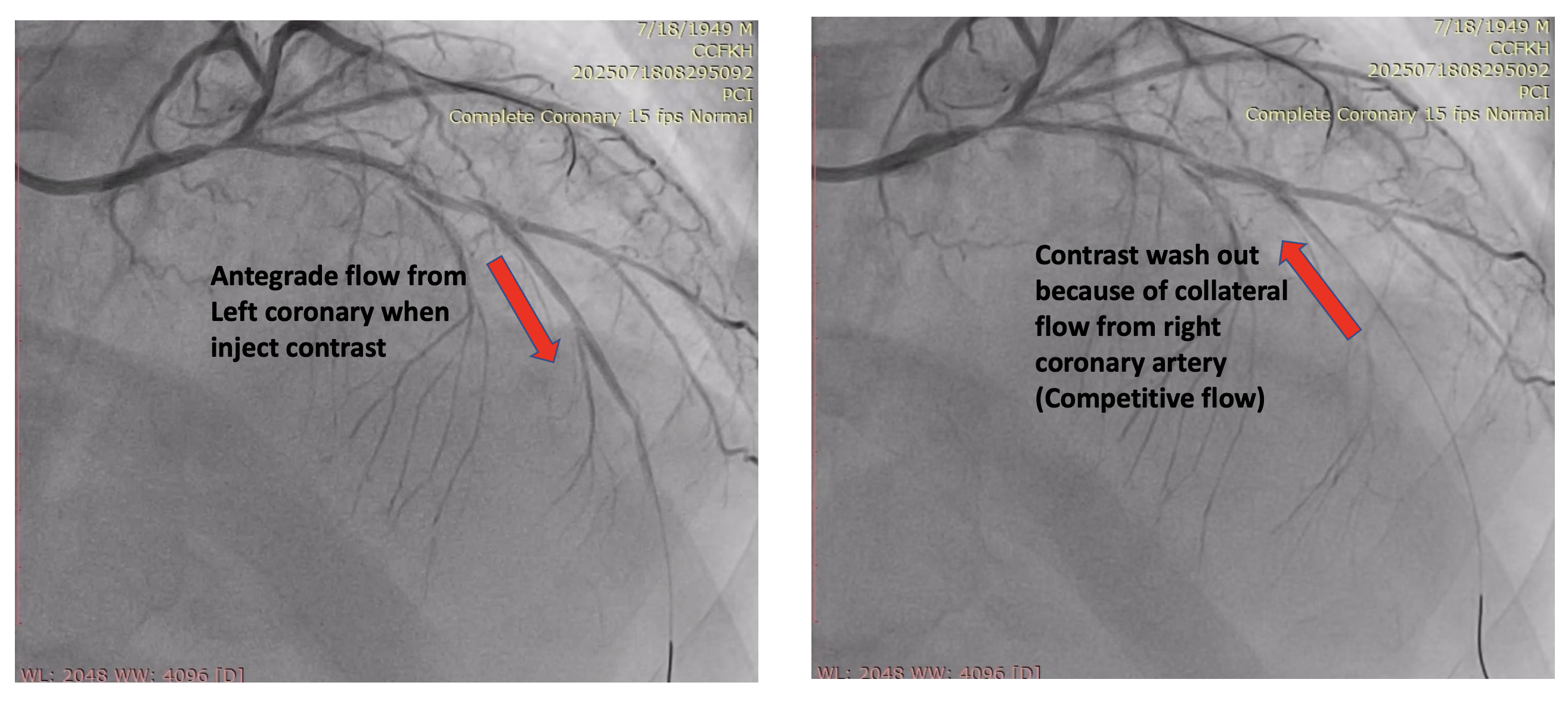
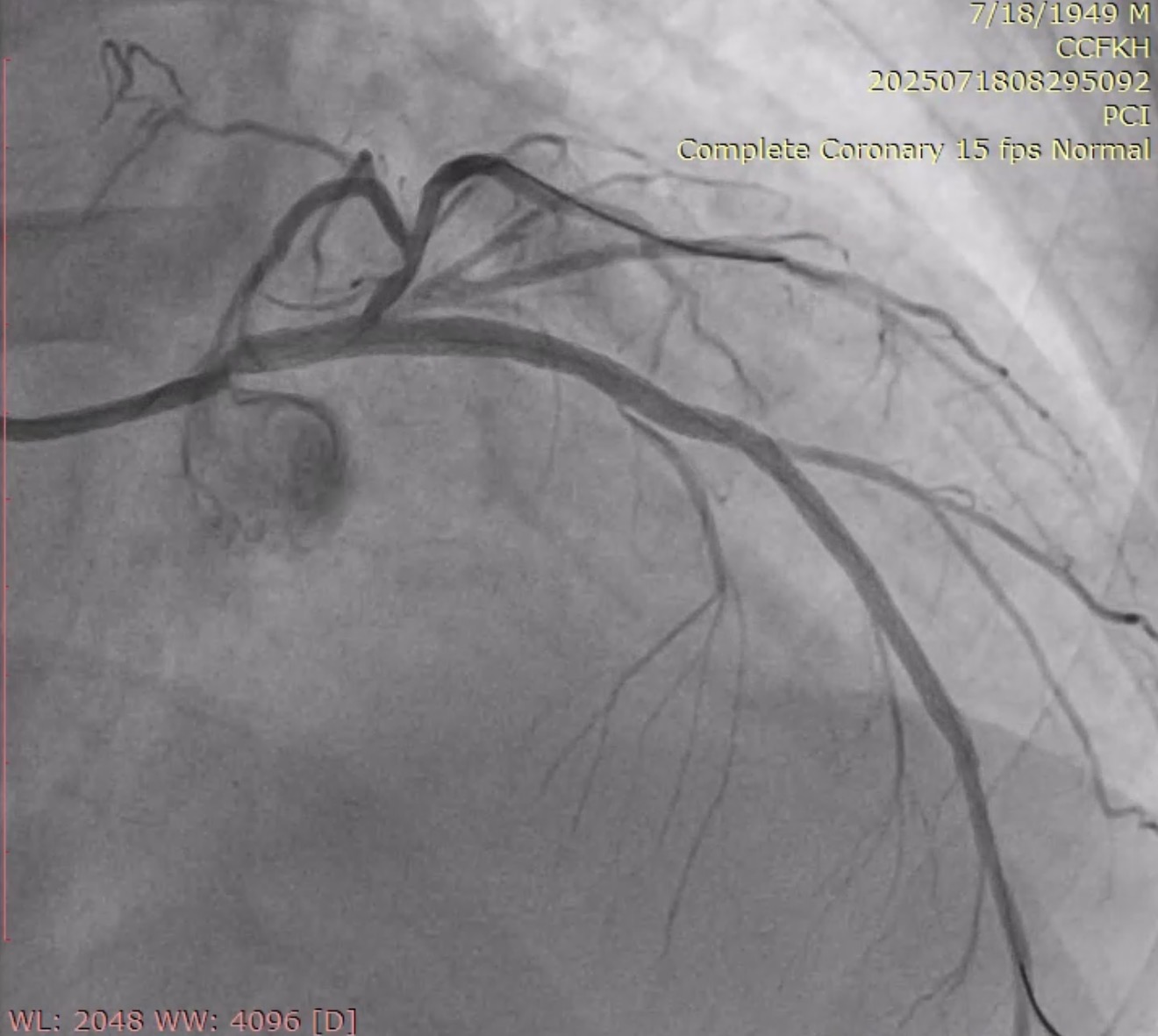
The left main was engaged by 6F EBU 3.5 via radial sheath. The LM occlusion was crossed by using workhorse guidewire (Cougar XT), suggesting an acute occlusion. Predilation with SC balloon (Sprinter Legend 1.5 x 12mm and Sprinter Legend 2.5 x 12mm) was performed at the occlusion site, resulting an antegrade flow from LM, but there was still no flow distally from mid-LAD.Plain old balloon angioplasty by Sprinter Legend 2.5 x 12mm performed at the mid-LAD, the flow from mid-LAD still was not achieved, giving the hypothesis of no reflow phenomenon. IC Nitroglycerine 100ug and IC Nicardipine 100ug were given several times, resulting a vasodilation and a better flow. It therefore revealed a significant competitive flow from powerful collaterals from the right coronary artery, ruling out the no reflow hypothesis (Refer to videos below for better illustration). Onyx Trucor DES 2.75 x 34mm, Onyx Trucor DES 3.0 x 22mm, and Onyx Trucor DES 3.5 x 22mm were implanted respectively from distal LAD to LM, and restored final TIMI 3 flow result

PCI1.mov
PCI2.mov
PCI3.mov
Case Summary
We report a rare case of sub-acute LMCA occlusion with excellent collateral flow from the right coronary system, resulting a stable hemodynamic status patient. The right coronary powerful collaterals flow created a competitive flow between left and right coronary system during left coronary intervention, which can imitate a no reflow phenomenon.