Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20250723_001
Coronary Artery Ruptured Due to Inappropriate Large Balloon – Rescued by Vascular Plug
By Saroj Kumar Sahoo, Ramachandra Barik, Debasis Acharya, Sai Karthik Kowtarapu, Subhas Pramanik, Saran Mohan, Sindhu Rao Malla
Presenter
Saroj Kumar Sahoo
Authors
Saroj Kumar Sahoo1, Ramachandra Barik1, Debasis Acharya1, Sai Karthik Kowtarapu1, Subhas Pramanik1, Saran Mohan2, Sindhu Rao Malla1
Affiliation
AIIMS Bhubaneswar, India1, AIIMS, Bhubaneswar, India2
View Study Report
CASE20250723_001
Coronary - Complication Management
Coronary Artery Ruptured Due to Inappropriate Large Balloon – Rescued by Vascular Plug
Saroj Kumar Sahoo1, Ramachandra Barik1, Debasis Acharya1, Sai Karthik Kowtarapu1, Subhas Pramanik1, Saran Mohan2, Sindhu Rao Malla1
AIIMS Bhubaneswar, India1, AIIMS, Bhubaneswar, India2
Clinical Information
Relevant Clinical History and Physical Exam
A 76-year-old man presented with exertional angina (NYHA class III) despite being onguideline-directed medical therapy. He experienced persistent symptoms, prompting furtherinvestigation. The patient had undergone PCI to the right coronary artery (RCA) two years prior for inferiorwall myocardial infarction and had since remained on regular medical therapy.
Relevant Test Results Prior to Catheterization
Routine blood investigations were normal. ECG showed no ST/T changes, and echocardiography indicated inferior wall hypokinesia with a left ventricular ejection fraction of 45%.
Relevant Catheterization Findings
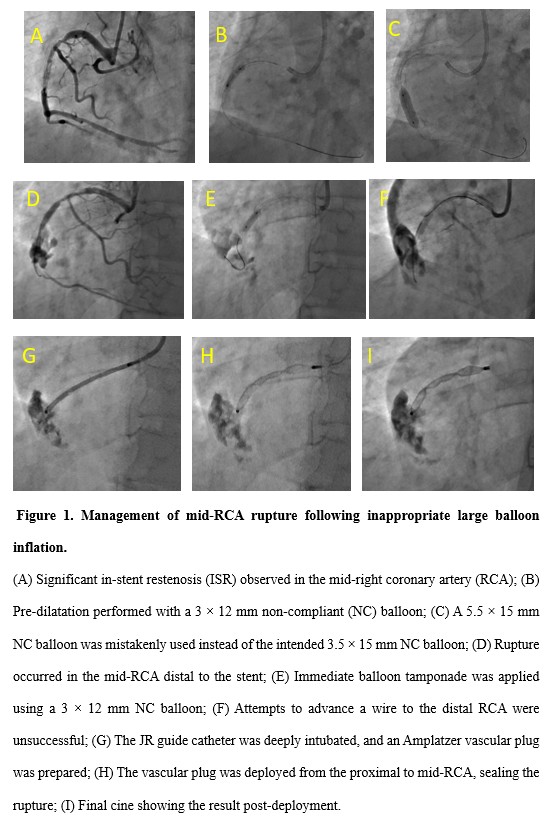
Coronary angiography revealed normal LAD and circumflex arteries, while RCA showed significant 80% in-stent restenosis (ISR) (Figure 1A; Video 1).
 Video 1 Baseline cine showing RCA ISR.mp4
Video 1 Baseline cine showing RCA ISR.mp4
Interventional Management
Procedural Step
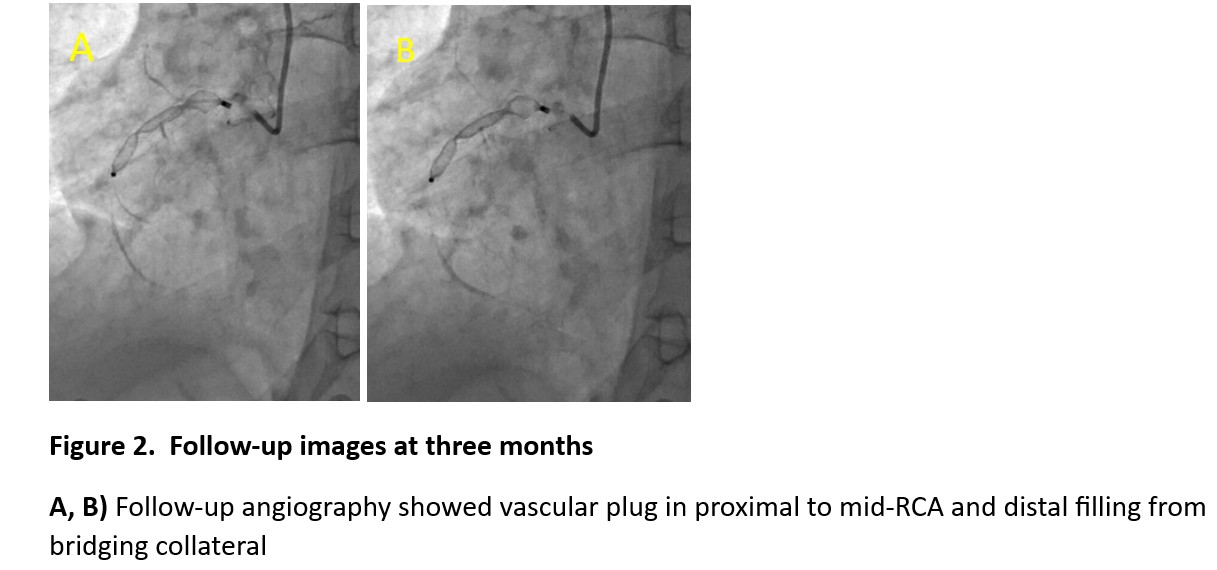
Given the significant ISRin the RCA, the plan was to treat it using a drug-eluting balloon (DEB). Initial pre-dilatation was performed with a 3 × 12 mmsemi-compliant (SC) balloon at 18 atm. (Figure 1B). As the stent size was 3.5mm, the plan was to proceed with a 3.5×15 mm non-compliant (NC) balloon beforeapplying the DEB. However, a 5.5 × 15 mm NC balloon was mistakenly selected(Figure 1C). Subsequent angiography confirmed the rupture. (Figure 1D). A 3 × 12mm balloon was immediately used for tamponade at 16 atm, and protamine sulfatewas administered to reverse heparin’s effects (Figure 1E). Despite multiple attempts, rewiring the distal RCA was unsuccessful, andthe wire entered the pericardium (Figure 1F). On-tableechocardiography confirmed mild pericardial effusion. Coil embolization wasdeemed unsuitable due to the artery’s size and rupture location. The onlyavailable option was to use a vascular plug. A9-AVP2-010 Amplatzer vascular plug was deployed in the proximal RCA to seal therupture. (Figure 1G-I) Following the procedure, the patient wasmonitored in the cardiac ICU, with serial echocardiograms confirming stablepericardial effusion. At three months, the angiography check revealed vascular plug in the RCA, with distal filling from bridging collaterals (Figure 2A, B).
Video 3 RCA Ruptured..mp4
Video 6. Vascular plug positioned..mp4
Video 7. Vascular Plug deployed.mp4
Case Summary
Coronary artery rupture due to hardware mismanagement is rare, emphasizing the importance of ensuring an appropriate device size. Although deploying a vascular plug saved the patient, preserving the native artery should always be prioritized if possible.