Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20250708_002
A Challenging Case of Dislodged Stent
By Quek Ao Xiang, Vicknesan A/L Kulasingham, Kwang How Ng, Hou Tee Lu, Gurudevan A/L Mahadevan
Presenter
Quek Ao Xiang
Authors
Quek Ao Xiang1, Vicknesan A/L Kulasingham1, Kwang How Ng1, Hou Tee Lu2, Gurudevan A/L Mahadevan1
Affiliation
Hospital Sultanah Aminah Johor Bahru, Malaysia1, Regency Specialist Hospital Johor , Malaysia2
View Study Report
CASE20250708_002
Coronary - Complication Management
A Challenging Case of Dislodged Stent
Quek Ao Xiang1, Vicknesan A/L Kulasingham1, Kwang How Ng1, Hou Tee Lu2, Gurudevan A/L Mahadevan1
Hospital Sultanah Aminah Johor Bahru, Malaysia1, Regency Specialist Hospital Johor , Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
A 41-year-old gentleman had underlying hypertension, diabetes mellitus and dyslipidemia diagnosed since 3 years ago. He had two vessels disease which involved the right coronary artery (RCA) and left anterior descending artery (LAD). He had percutaneous coronary intervention (PCI) done to LAD 7 months ago. He was electively admitted for staged PCI to RCA. His blood pressure on admission was 132/76mmHg and a pulse of 83 bpm. The other physical examinations were unremarkable.
Relevant Test Results Prior to Catheterization
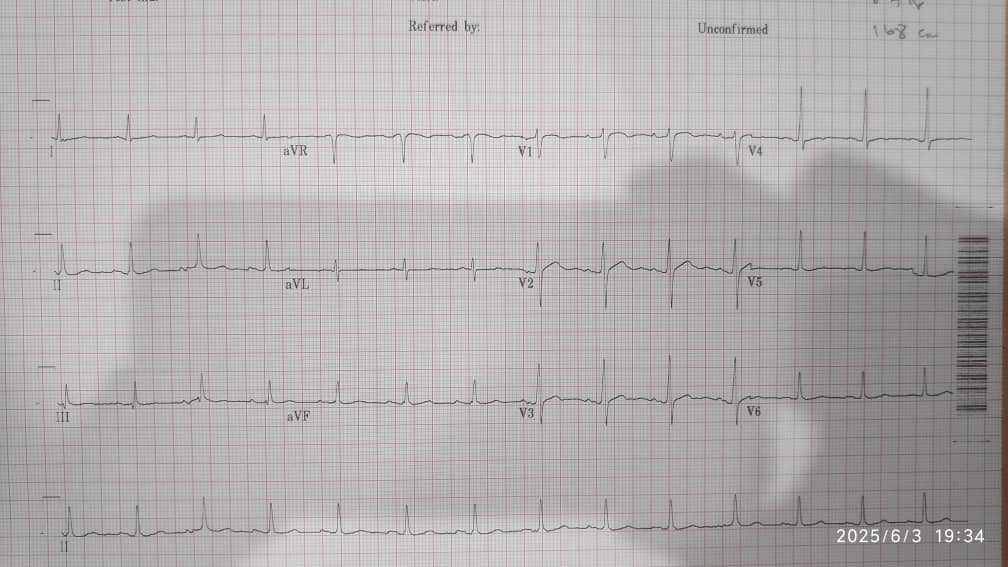
The full blood count was normal. Hemoglobin was 13.7 g/L, white blood cell was 12.2 (10^9/L) and platelet was 332 (10^9/L). The renal profile was normal with urea of 4.1 mmol/L and creatinine of 66 µmol/L. The total cholesterol was 2.4 mmol/L. The random blood glucose was elevated at 19.3 mmol/L. The electrocardiogram (ECG) showed sinus rhythm and no acute ischemic changes. The echocardiogram showed left ventricular ejection fraction of 50-55% with normal chamber size.
Relevant Catheterization Findings
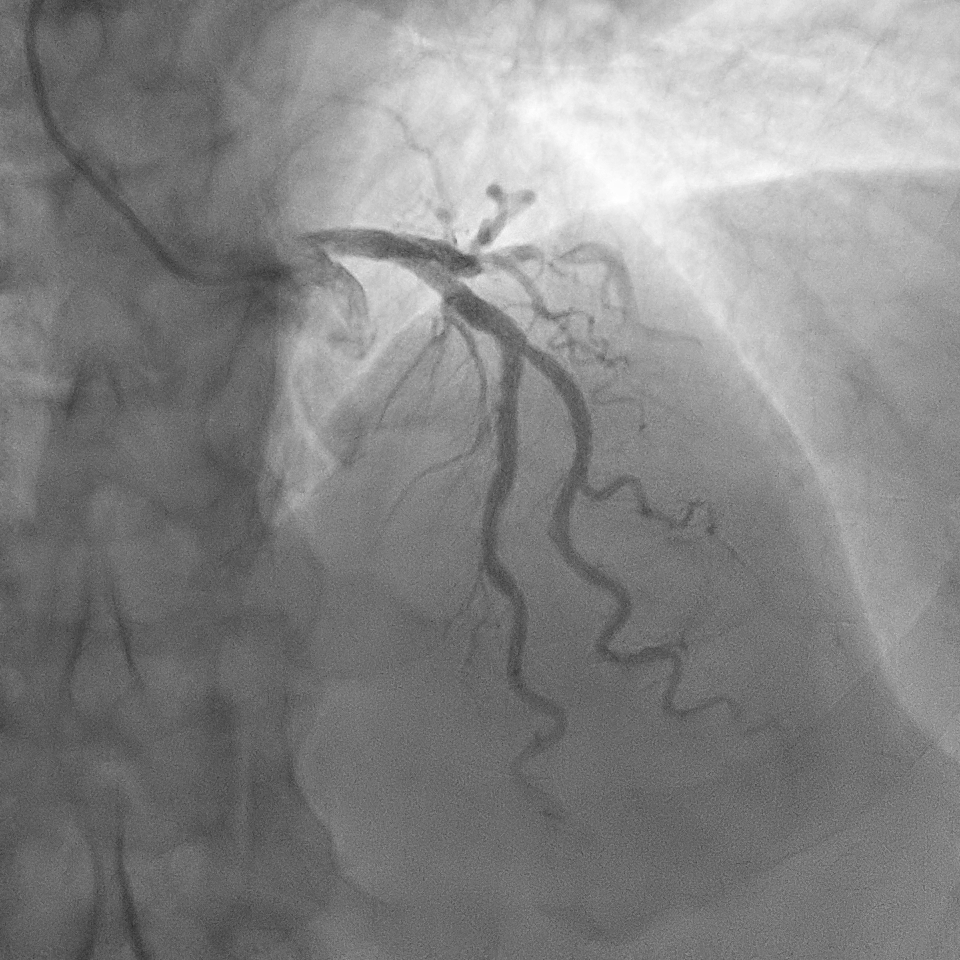
The angiogram showed right dominant system. The left main coronary artery was normal. The left anterior descending (LAD) stent was patent. There was a severe discrete stenosis at obtuse marginal branch (OM1). There was severe stenosis at mid right coronary artery (RCA) and moderate stenosis at proximal RCA.
 MOVIE-0015.mp4
MOVIE-0015.mp4
MOVIE-0016.mp4
MOVIE-0017.mp4
Interventional Management
Procedural Step
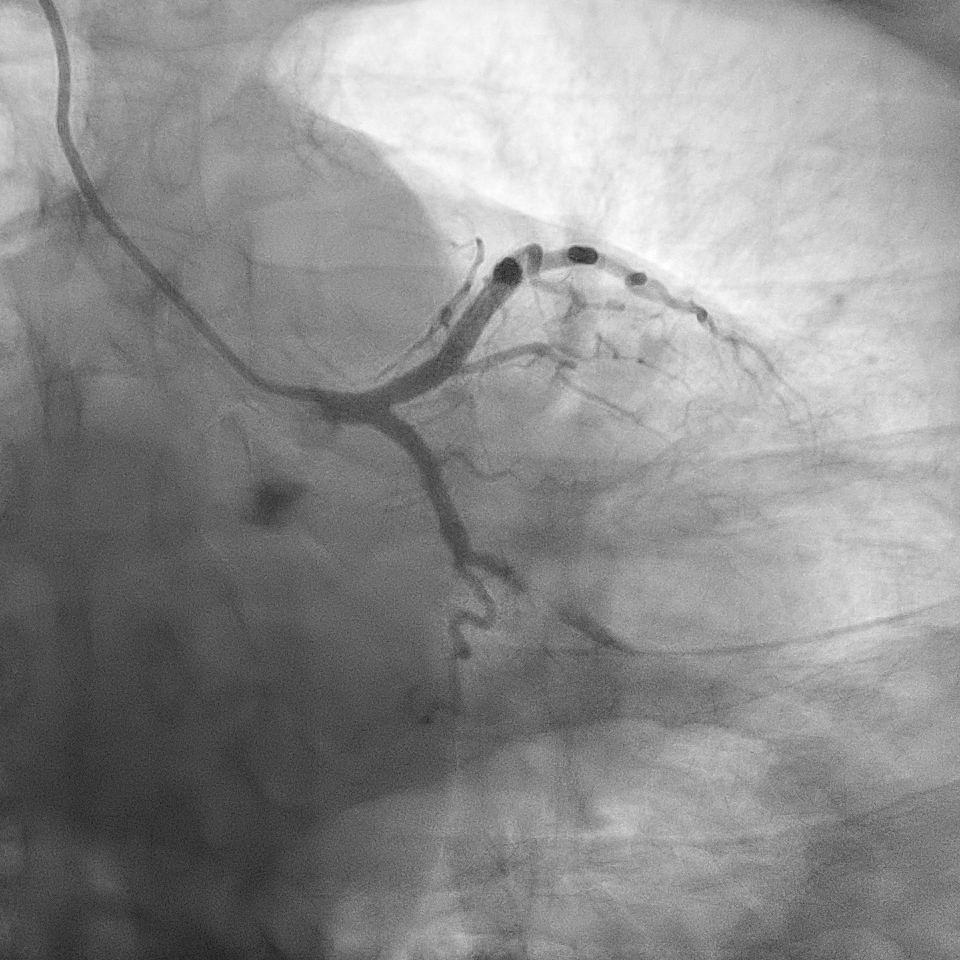
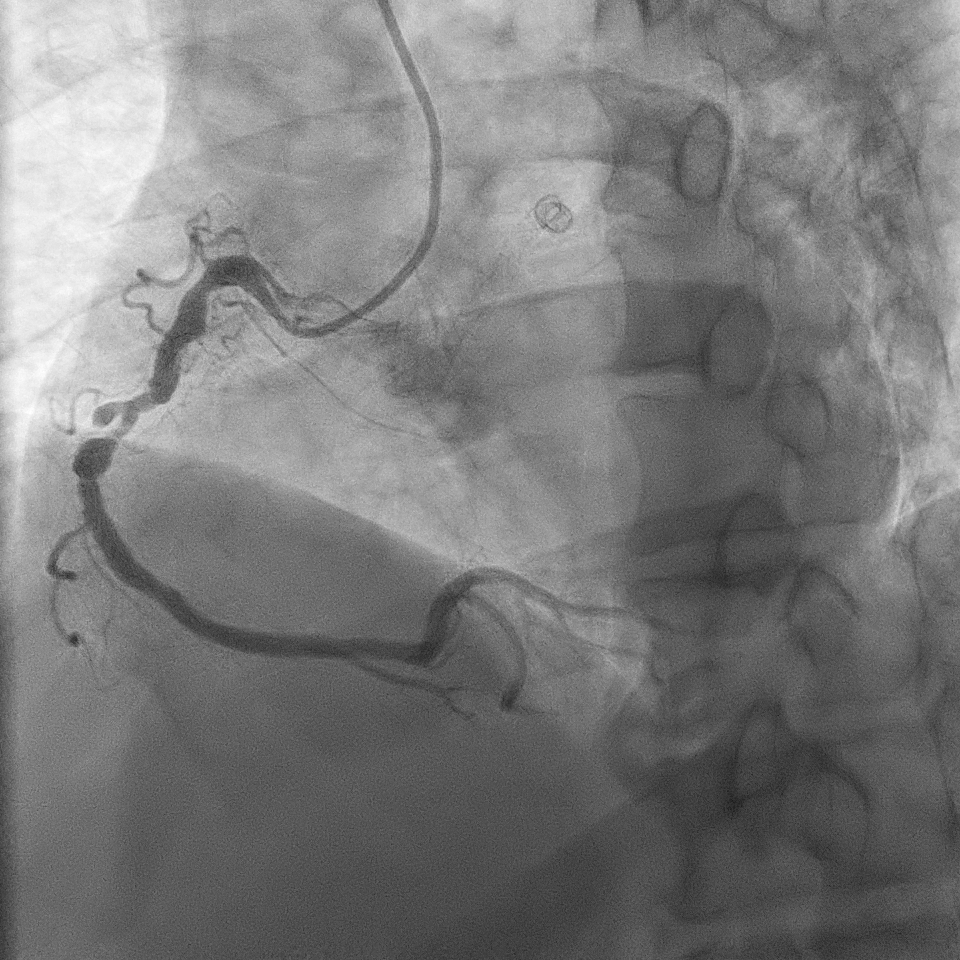
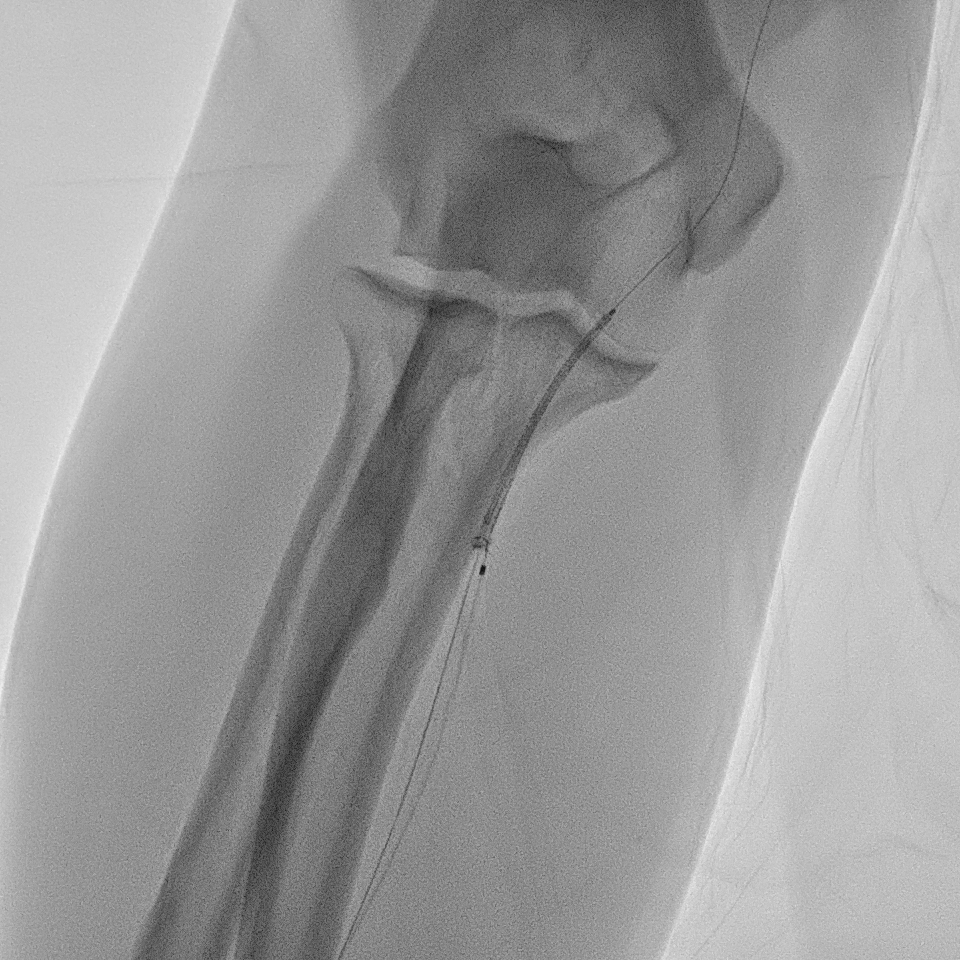
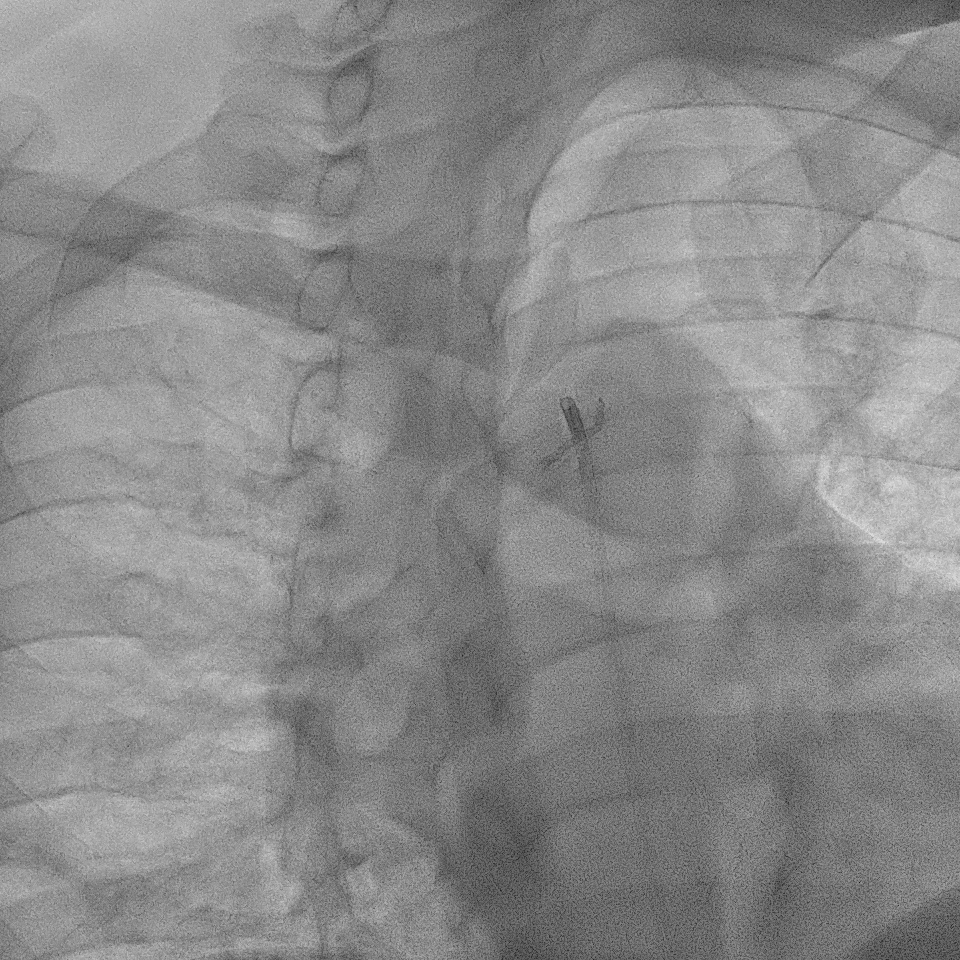
A right radial artery approach with 6Fr sheath was used. The right coronary system was engaged with 6Fr Judkin Right (JR4) guiding catheter. The posterior left ventricular branch was wired with Runthrough NS. Intravascular ultrasound (IVUS) showed distal RCA landing zone vessel size of 4.0-4.5mm in diameter. The mid RCA showed minimal luminal area (MLA) of 1.95mm2 with fibrous plaque and calcification at 12 o'clock. The proximal RCA landing vessel size was 4.5-5.0mm in diameter. The lesion was predilated with NC Trek Neo balloon 3.0x15mm. Attempted multiple times to deliver the stent SYNERGY 4.0X48mm but failed. The stent could not be passed into proximal RCA and eventually the distal stent edge crimpled and unable to be withdrawn into the guiding catheter. Tried to pull back system enbloc into the radial artery. Attempted to pull the stent into guider but failed again. The guiding catheter was removed. The stent was left with coronary wire in situ. Exchanged 6Fr radial sheath to slender sheath and attempted to snare stent with 2.0mm snare but failed. Attempted multiple wire wrapping technique with 3 BMW wires but failed. Decided to puncture right femoral artery with 8Fr sheath. A 7Fr JR4 guiding catheter was introduced into right brachial artery. A 7mm snare then snared the stent and removed it via femoral. The lesion was predilated with Scoreflex 3.5x20mm, stented with Supraflex Cruz 4.0x48mm and post-dilated with NC balloon 4.5mm. Result was TIMI 3 and no dissection.

MOVIE-0018.mp4
MOVIE-0019.mp4
MOVIE-0001.mp4
Case Summary
Several factors had led to difficult in delivering the stent into RCA in this case. The lesion was not adequately prepared before stenting. Besides, the curvy or tortuous anatomy of RCA may contribute to this problem especially when using long stent. When encounter resistance during stent delivery, is crucial to avoid forceful pushing to prevent stent from being damaged or dislodged. Guide extension can be used to assist in stent delivery. This case demonstrated few techniques in retrieving the dislodged and crimpled stent. These include the use of snaring tools via the radial or femoral artery as well as the multiple wire wrapping technique.