Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251114_0013
Percutaneous Coronary Intervention Versus Optimal Medical Therapy for Chronic Total Occlusion: A Meta-Analysis From Viability Perspective
By Hendy Bhaskara Perdana Putra
Presenter
Hendy Bhaskara Perdana Putra
Authors
Hendy Bhaskara Perdana Putra1
Affiliation
Cilacap Military Naval Base, Indonesia1
View Study Report
ABS20251114_0013
CTO
Percutaneous Coronary Intervention Versus Optimal Medical Therapy for Chronic Total Occlusion: A Meta-Analysis From Viability Perspective
Hendy Bhaskara Perdana Putra1
Cilacap Military Naval Base, Indonesia1
Background
Chronic Total Occlusion (CTO) continues to represent a significant challenge in interventional cardiology. Although numerous studies have been conducted, whether percutaneous coronary intervention (PCI) or optimal medical therapy (OMT) remains elusive. While several meta-analyses have been performed to date, virtually no one evaluated outcomes through the perspective of myocardial viability.
Methods
We performed a systematic literature search from several electronic databases. We used keyword “chronic total occlusion” and “percutaneous coronary intervention” or “optimal medical therapy”. The inclusion criteria were studies which comparing percutaneous coronary intervention and optimal medical therapy in CTO lesion, either randomized or non – randomized was accepted. The primary endpoints were all cause mortality and cardiac death. Secondary endpoints were MACE, myocardial infarction, any revascularization and stroke. Risk ratio (RR) with 95% confidence intervals (CIs) were used to report all outcomes.
Results
A total of eightteen studies were selected with total 11.410 patients were pooled in our analysis. 6.292 patients in PCI group and 5.118 patients in OMT group.
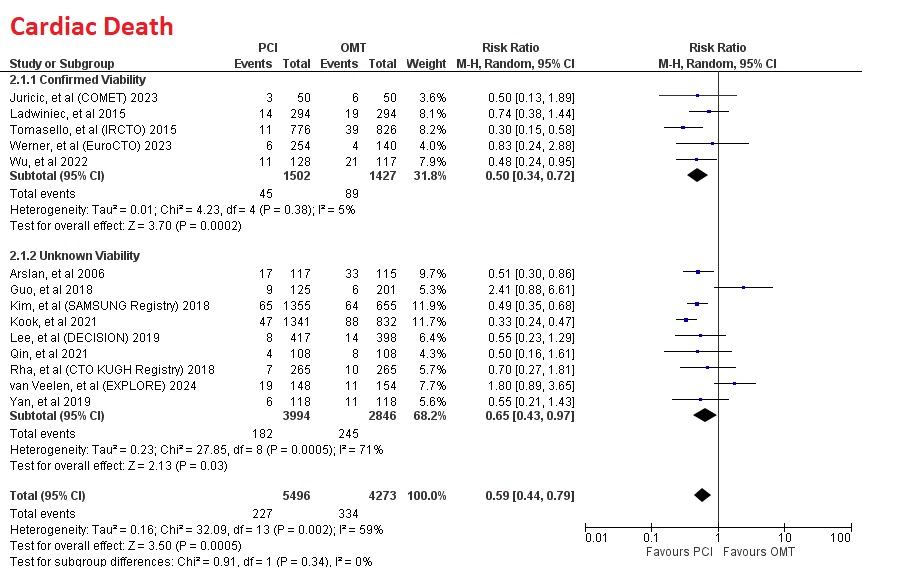
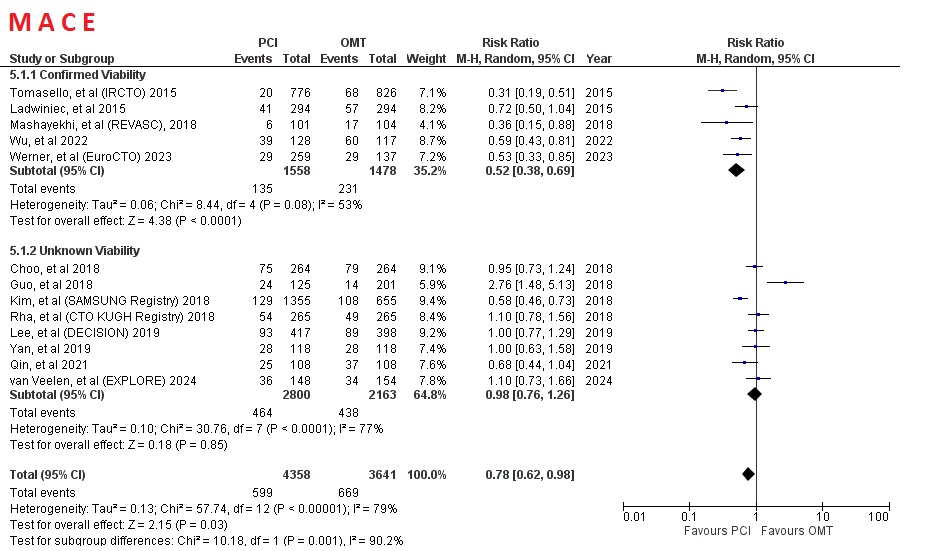
Compared to immediate OMT, overall PCI significantly reduce all cause death (RR=0.62 [95% CI, 0.49-0.77], p<0.0001), cardiac death (RR=0.59 [95% CI, 0.44-0.79], p=0.0005) and MACE (RR=0.78 [95% CI, 0.62-0.98], p=0.03).
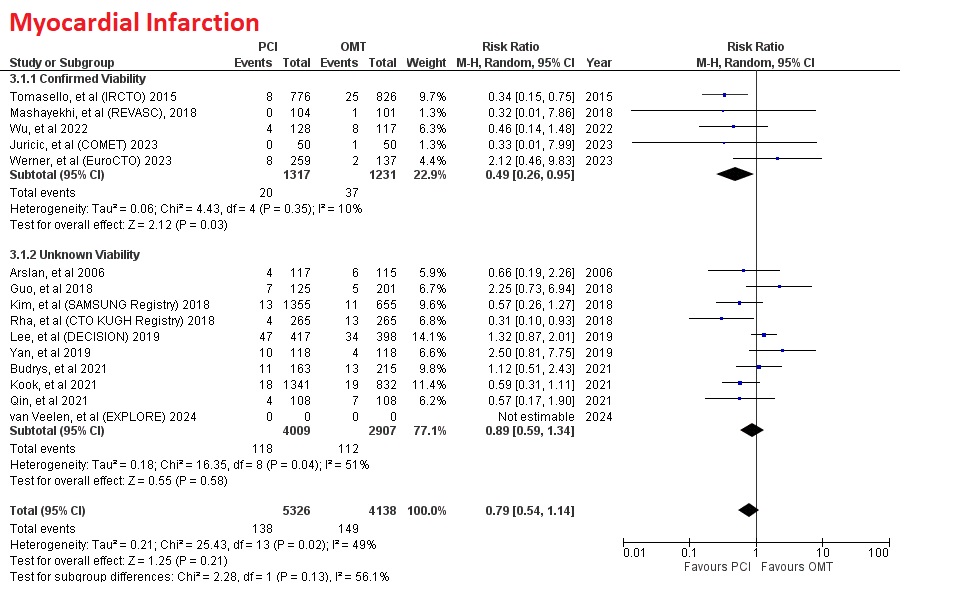
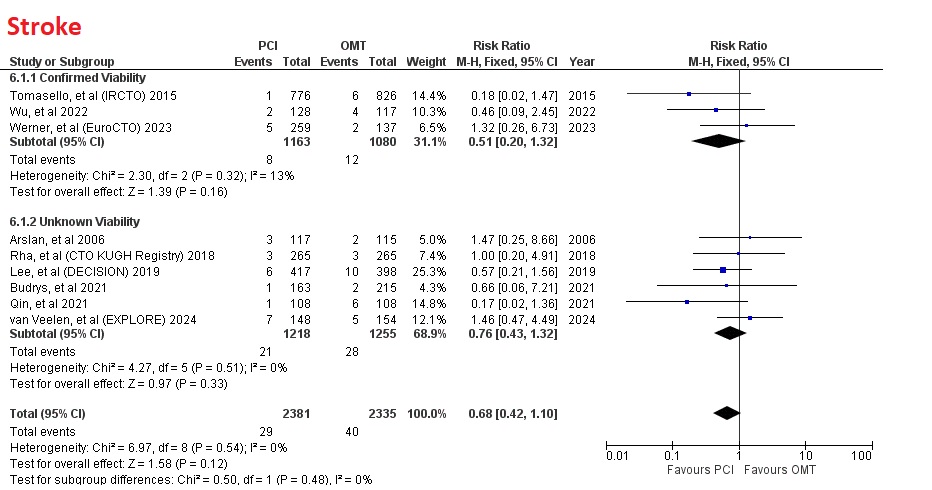
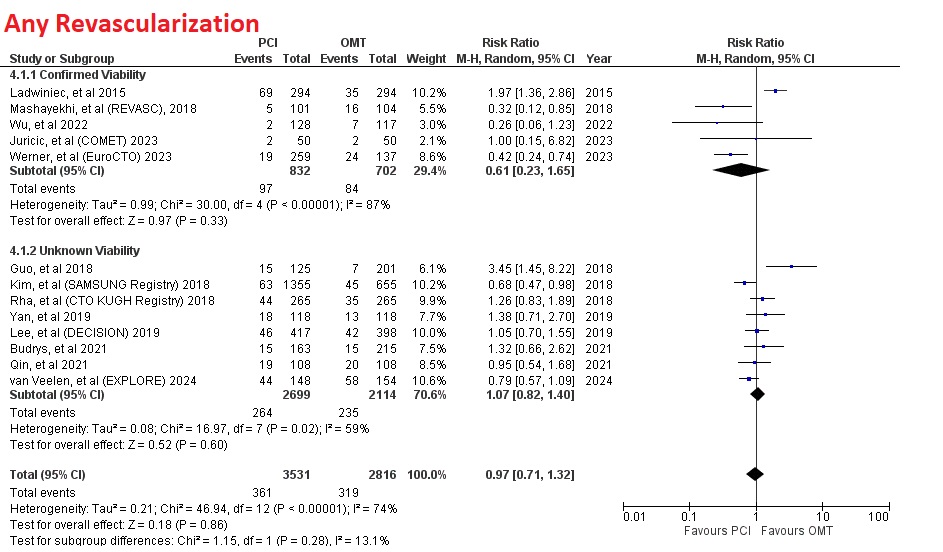
However, PCI had no significant difference in myocardial infarction (RR=0.79 [95% CI, 0.54-1.14], p=0.21), any revascularization (RR=0.97 [95% CI, 0.71-1.32], p=0.86), and stroke (RR=0.68 [95% CI, 0.42-1.10], p=0.12)
Interestingly, subgroup of studies which performed viability test before PCI had more significant result compar ed to subgroup who did not. Compared to subgroup which do not mandatory viability test, subgrouup which confirmed myocardial viability had more significant reduction in MACE (RR=0.52 [95% CI, 0.38-0.69], p<0.0001) versus (RR=0.98 [95% CI, 0.76-1.26], p=0.85) and myocardial infarction (RR=0.49 [95% CI, 0.26-0.95], p=0.03) versus (RR=0.89 [95% CI, 0.59-1.34], p=0.58)
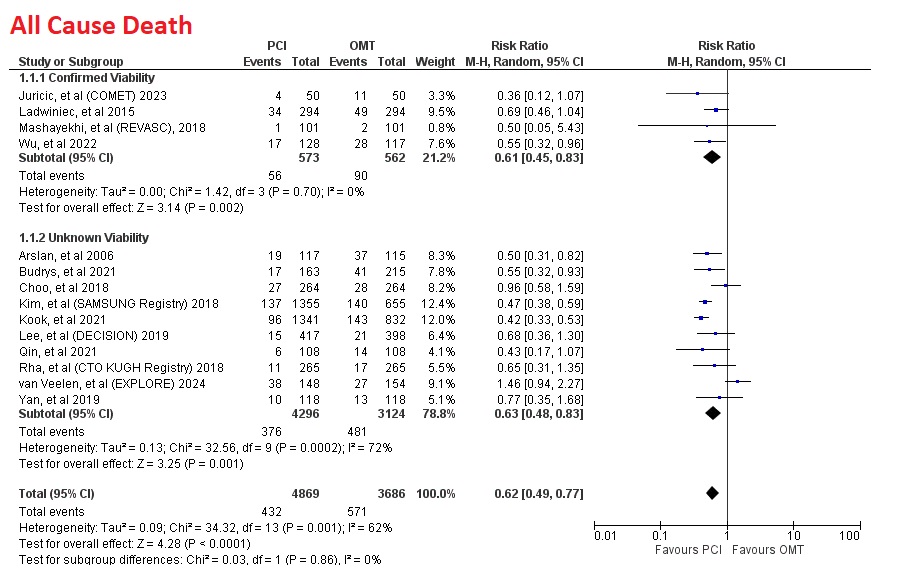
Compared to immediate OMT, overall PCI significantly reduce all cause death (RR=0.62 [95% CI, 0.49-0.77], p<0.0001), cardiac death (RR=0.59 [95% CI, 0.44-0.79], p=0.0005) and MACE (RR=0.78 [95% CI, 0.62-0.98], p=0.03).
However, PCI had no significant difference in myocardial infarction (RR=0.79 [95% CI, 0.54-1.14], p=0.21), any revascularization (RR=0.97 [95% CI, 0.71-1.32], p=0.86), and stroke (RR=0.68 [95% CI, 0.42-1.10], p=0.12)
Interestingly, subgroup of studies which performed viability test before PCI had more significant result compar ed to subgroup who did not. Compared to subgroup which do not mandatory viability test, subgrouup which confirmed myocardial viability had more significant reduction in MACE (RR=0.52 [95% CI, 0.38-0.69], p<0.0001) versus (RR=0.98 [95% CI, 0.76-1.26], p=0.85) and myocardial infarction (RR=0.49 [95% CI, 0.26-0.95], p=0.03) versus (RR=0.89 [95% CI, 0.59-1.34], p=0.58)
Conclusion
PCI significantly yields better outcomes compared to OMT, particularly in studies that confirm myocardial viability prior to PCI, showing significantly lower rates of all-cause death, cardiac death, MACE, and myocardial infarction than studies without assessment of myocardial viability. Confirming myocardial viability before PCI may become a game-changer in determining which therapy, PCI or OMT is more appropriate.