Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251114_0008
Uncovering the Fatal Signal: Early Il-6 Measurement Predicts Mortality in Acute Decompensated Heart Failure
By Amalia Adityas Dyah Safitri, Bernadhet Daisy Kenconosari, Raditya Widyo Ananto, Dyah Samti Mayasari, Ira Puspitawati, Riswan Hadi Kusuma, Anggoro Budi Hartopo, Salvatore Di Somma
Presenter
Amalia Adityas Dyah Safitri
Authors
Amalia Adityas Dyah Safitri1, Bernadhet Daisy Kenconosari1, Raditya Widyo Ananto1, Dyah Samti Mayasari1, Ira Puspitawati1, Riswan Hadi Kusuma2, Anggoro Budi Hartopo1, Salvatore Di Somma3
Affiliation
Sardjito Hospital, Indonesia1, UGM Academic Hospital, Indonesia2, Great Network, Italy3
View Study Report
ABS20251114_0008
Vascular Heart Disease and Cardiomyopathies
Uncovering the Fatal Signal: Early Il-6 Measurement Predicts Mortality in Acute Decompensated Heart Failure
Amalia Adityas Dyah Safitri1, Bernadhet Daisy Kenconosari1, Raditya Widyo Ananto1, Dyah Samti Mayasari1, Ira Puspitawati1, Riswan Hadi Kusuma2, Anggoro Budi Hartopo1, Salvatore Di Somma3
Sardjito Hospital, Indonesia1, UGM Academic Hospital, Indonesia2, Great Network, Italy3
Background
Acute heart failure (AHF) remains a major cause of in-hospital morbidity and mortality, emphasizing the importance of timely risk assessment. Elevated IL-6 levels have been linked to adverse outcomes. This study evaluated the prognostic value of admission IL-6 levels in predicting in-hospital mortality among patients presenting with AHF
Methods
Patients aged more than 18 years presenting with ADHF (excluding acute coronary syndrome) were prospectively enrolled from the emergency departments of two referral hospitals in Yogyakarta, Indonesia. Serum IL-6 was measured at admission, and all patients received standard heart failure therapy. In-hospital mortality was defined as the primary outcome. Optimal IL-6 cut-off values were determined using Youden’s J index. Associations between IL-6 and in-hospital mortality were evaluated using multivariate logistic regression adjusted for clinical and laboratory covariates, and survival differences were further examined with Kaplan–Meier and Cox proportional hazards analyses
Results
A total of 268 patients with ADHF were included, of whom 31 died during hospitalization. After adjustment for clinical and laboratory covariates (age, sex, BMI, LVEF, SBP, WBC count, uric acid, creatinine, hs-troponin I, andNT-proBNP), IL-6 more than 31 pg/mL was associated with a significantly higher risk of in-hospital mortality (OR 6.20; 95% CI 1.99–19.28; p = 0.002). Kaplan–Meier analysis showed shorter survival in this group, with a mean survival of 24.2 days (95% CI 22.1–26.3; log-rank <0.001). Cox regression confirmed this association, with elevated IL-6 linked to an increased hazard of in-hospital mortality (HR ≈ 5; p = 0.001), indicating a strong relationship with earlier death. The clear association between elevated IL-6 and early in-hospital mortality highlights its role as a marker of heightened inflammatory stress in ADHF. Its consistent predictive performance across models suggests that IL-6 can reliably identify patients at imminent risk, enabling clinicians to prioritize early monitoring and consider more targeted therapeutic strategies.
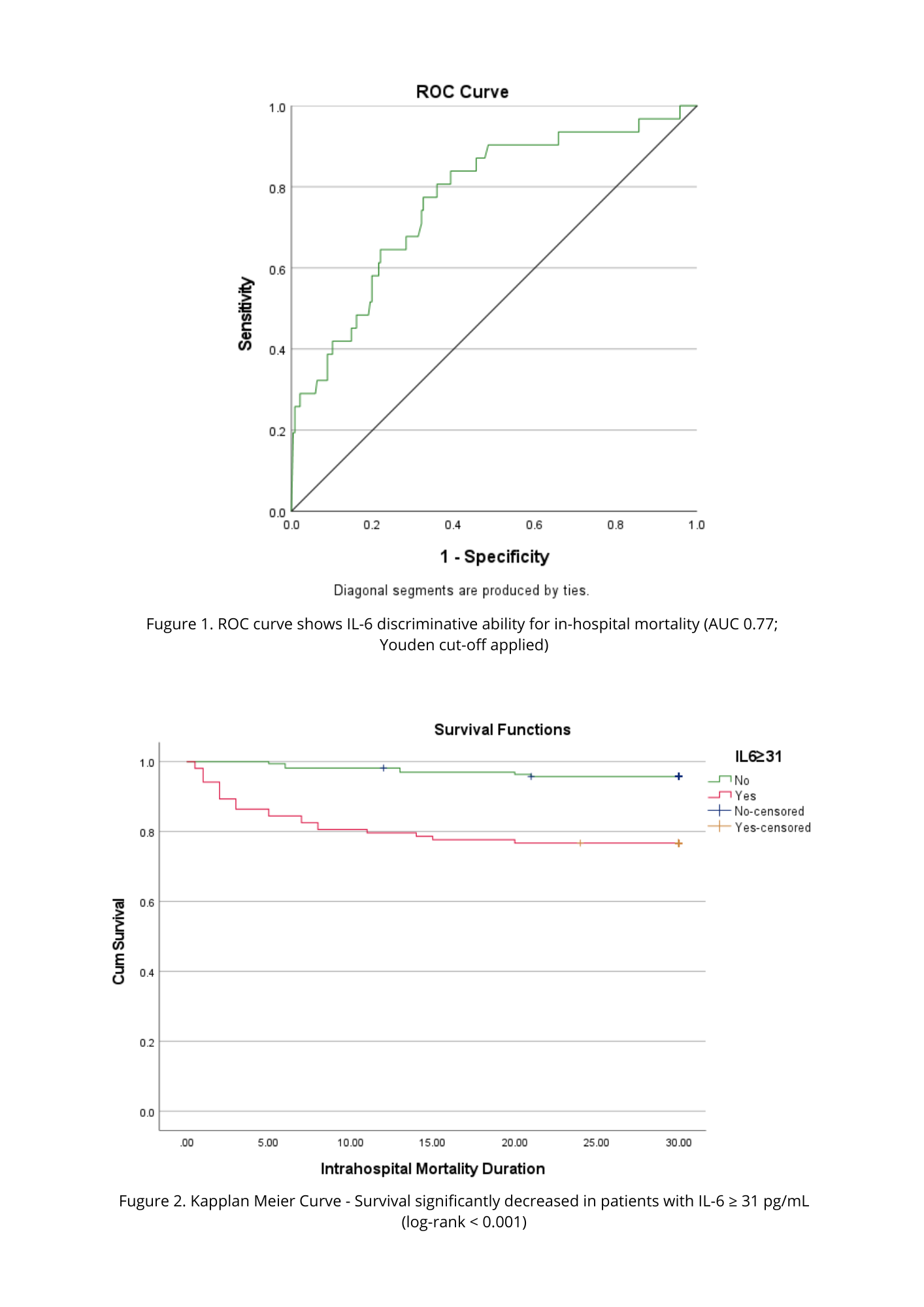
Conclusion
IL-6 more than 31 pg/mL consistently identified patients at markedly higher risk of early in-hospital mortality, underscoring its value as a prognostic marker in ADHF. These findings support the use of admission IL-6 measurement to enhance early risk stratification and guide clinical decision-making.