Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251113_0001
Mechanical Thrombectomy Using Rotarex®: Enhanced Outcomes Through Hounsfield Unit-Guided Case Selection
By Junyong Jekal, Sang-Su Lee
Presenter
Sang-Su Lee
Authors
Junyong Jekal1, Sang-Su Lee2
Affiliation
Pusan National University Yang San Hospital , Korea (Republic of)1, PusanNational University Yang San Hospital , Korea (Republic of)2
View Study Report
ABS20251113_0001
Thrombus Removal Devices and Techniques
Mechanical Thrombectomy Using Rotarex®: Enhanced Outcomes Through Hounsfield Unit-Guided Case Selection
Junyong Jekal1, Sang-Su Lee2
Pusan National University Yang San Hospital , Korea (Republic of)1, PusanNational University Yang San Hospital , Korea (Republic of)2
Background
Background:
The Rotarex™ mechanical thrombectomy system has demonstrated efficient removal ofthrombus but outcomes vary across studies. We hypothesize that preoperativeanalysis of thrombus Hounsfield Unit (HU) on CT angiography may enhance patientselection and contribute to superior outcomes.
Methods:
This retrospective study analyzed 14 cases of lower extremity arterialthrombosis treated with Rotarex™ at our institution. All patients underwent CT-basedHU analysis of thrombus prior to intervention. Clinical outcomes, Rutherfordclassification, ankle-brachial index (ABI), and perioperative laboratory data(RBC, hemoglobin, total bilirubin) were evaluated.
Results:
Technical success was achieved in 100% of cases. Mean preoperative HU ofthrombus was 60.4±2.9. ABI improved significantly from 0.51±0.23 to 0.83±0.17. Rutherfordstage improved in all cases. Postoperative labvalues showed a modest decrease in RBC (–0.17±0.20×10⁶/μL), hemoglobin (–0.42±0.57g/dL), and a significant increase in total bilirubin (+0.22±0.25 mg/dL, p = 0.0138). No major complications such as distalembolization or vascular rupture occurred.
Conclusion:
HU analysis of thrombus may help select suitable candidates for mechanicalthrombectomy using Rotarex™, potentially improving technical success andminimizing complications. Our outcomes compare favorably to prior literature,supporting the integration of HU-based planning into clinical workflows.
미디어1.mp4
미디어3.mp4
The Rotarex™ mechanical thrombectomy system has demonstrated efficient removal ofthrombus but outcomes vary across studies. We hypothesize that preoperativeanalysis of thrombus Hounsfield Unit (HU) on CT angiography may enhance patientselection and contribute to superior outcomes.
Methods:
This retrospective study analyzed 14 cases of lower extremity arterialthrombosis treated with Rotarex™ at our institution. All patients underwent CT-basedHU analysis of thrombus prior to intervention. Clinical outcomes, Rutherfordclassification, ankle-brachial index (ABI), and perioperative laboratory data(RBC, hemoglobin, total bilirubin) were evaluated.
Results:
Technical success was achieved in 100% of cases. Mean preoperative HU ofthrombus was 60.4±2.9. ABI improved significantly from 0.51±0.23 to 0.83±0.17. Rutherfordstage improved in all cases. Postoperative labvalues showed a modest decrease in RBC (–0.17±0.20×10⁶/μL), hemoglobin (–0.42±0.57g/dL), and a significant increase in total bilirubin (+0.22±0.25 mg/dL, p = 0.0138). No major complications such as distalembolization or vascular rupture occurred.
Conclusion:
HU analysis of thrombus may help select suitable candidates for mechanicalthrombectomy using Rotarex™, potentially improving technical success andminimizing complications. Our outcomes compare favorably to prior literature,supporting the integration of HU-based planning into clinical workflows.
미디어1.mp4
미디어3.mp4
Methods
Methods: Thisretrospective study analyzed 14 patients with lower extremity arterialocclusion who underwent mechanical thrombectomy using Rotarex™ between March2025 to July 2025 at Pusan national university Yangsan hospital. All patientshad contrast-enhanced CT angiography prior to the procedure. As this was aretrospective study, it was exempt from IRB review.
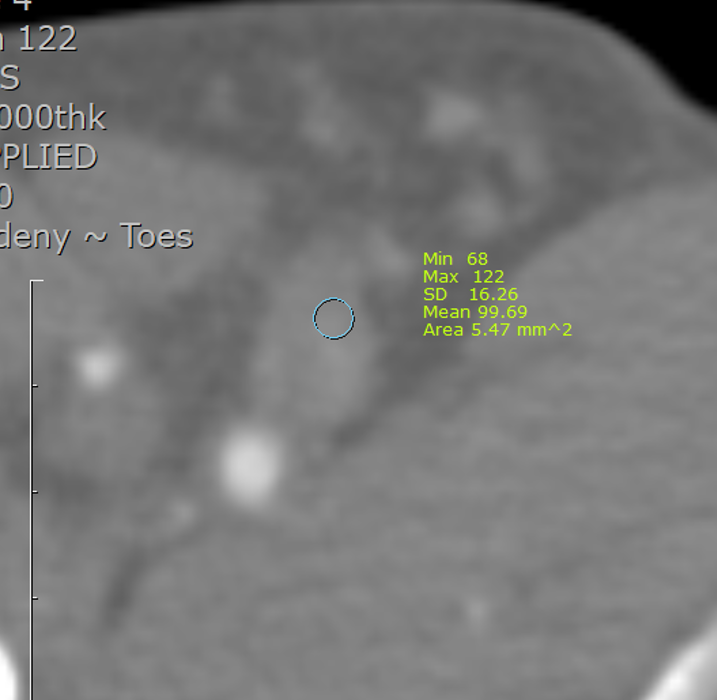
Thrombus HU values were measured using standardized regions of interest (ROI)within the occluded vessel segments. Additional clinical data included patientdemographics, type of thrombus, in-stent vs native thrombosis, and lesionlength. The type of thrombus was classified as acute if it lasted less than 2weeks, subacute if it lasted between 2 weeks and 2 months, and chronic if itlasted more than 2 months based on the patient's history.
Procedures were performed under general anesthesia using 8F Rotarex™ device. Balloon angioplasty and adjunctive stenting were selectivelyperformed. Clinical endpoints included technical success, Rutherford stagechange, ABI, and changes in laboratory parameters (RBC, hemoglobin, totalbilirubin).
Thrombus HU values were measured using standardized regions of interest (ROI)within the occluded vessel segments. Additional clinical data included patientdemographics, type of thrombus, in-stent vs native thrombosis, and lesionlength. The type of thrombus was classified as acute if it lasted less than 2weeks, subacute if it lasted between 2 weeks and 2 months, and chronic if itlasted more than 2 months based on the patient's history.
Procedures were performed under general anesthesia using 8F Rotarex™ device. Balloon angioplasty and adjunctive stenting were selectivelyperformed. Clinical endpoints included technical success, Rutherford stagechange, ABI, and changes in laboratory parameters (RBC, hemoglobin, totalbilirubin).
Results
All 14 patientsunderwent mechanical thrombectomy with the Rotarex™ system and achievedsuccessful revascularization of the target vessel, corresponding to a 100%technical success rate. Flow restoration was obtained in a single session inevery case, without the need for catheter-directed thrombolysis or opensurgical conversion.
Conclusion
Conclusion: Ourinstitutional experience demonstrates that mechanical thrombectomy withRotarex® can be highly successful when guided by HU-based thrombuscharacterization. This novel approach may improve patient selection, reduce thelikelihood of procedural failure, and offer insights into thrombus fragility.Further multicenter studies are needed to validate HU thresholds and to refineselection criteria for optimal mechanical thrombectomy candidates.