Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251111_0005
Half-Dose Pharmaco-Invasive Strategy as an Alternative Reperfusion Approach for ST-Elevation Myocardial Infarction: Evidence From a Systematic Review and Network Meta-Analysis
By Khansa Maria Salsabila, Nahar Taufiq, Arditya Damar Kusuma
Presenter
Khansa Maria Salsabila
Authors
Khansa Maria Salsabila1, Nahar Taufiq1, Arditya Damar Kusuma1
Affiliation
Department of Cardiology and Vascular Medicine, Dr. Sardjito General Hospital, Yogyakarta, Indonesia1
View Study Report
ABS20251111_0005
ACS/AMI
Half-Dose Pharmaco-Invasive Strategy as an Alternative Reperfusion Approach for ST-Elevation Myocardial Infarction: Evidence From a Systematic Review and Network Meta-Analysis
Khansa Maria Salsabila1, Nahar Taufiq1, Arditya Damar Kusuma1
Department of Cardiology and Vascular Medicine, Dr. Sardjito General Hospital, Yogyakarta, Indonesia1
Background
Prompt reperfusion is vital in ST-elevation myocardial infarction (STEMI) to improve survival, yet primary PCI (PPCI) remains less accessible in low-resource regions. Fibrinolysis offers wider availability but carries higher bleeding risk. The half-dose pharmaco-invasive (PI) strategy, combining half-dose fibrinolysis followed by PCI within 24 hours, has emerged as a practical alternative. This study aimed to evaluate outcomes of half-dose PI compared with full-dose PI and PPCI to identify the optimal reperfusion strategy where 24/7 access is limited
Methods
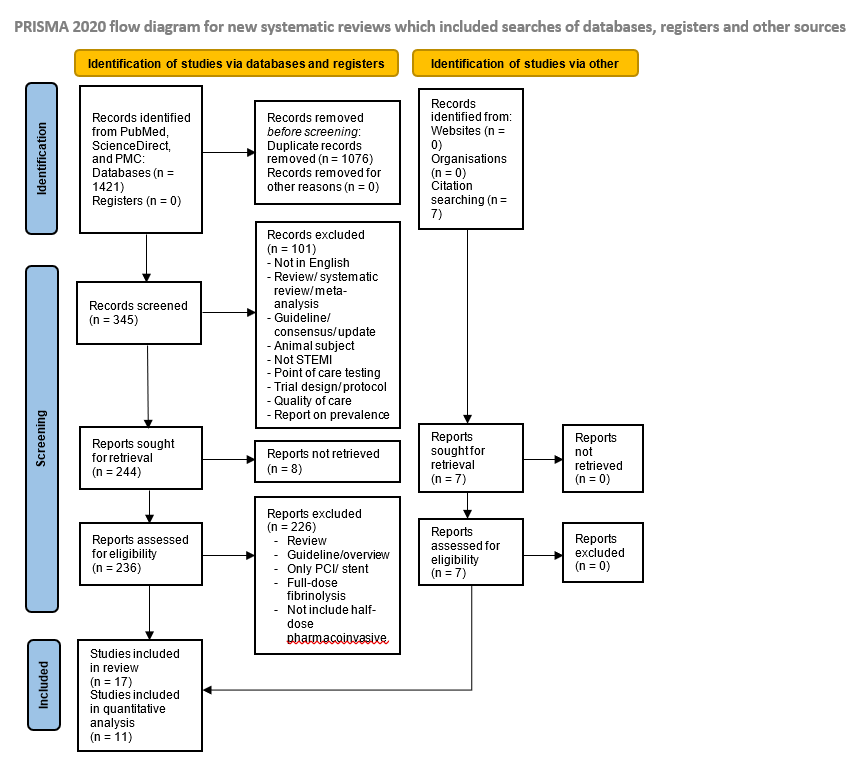
A systematic literature search following PRISMA guidelines was conducted across PubMed, PMC, and ScienceDirect for studies (2003-2025) evaluating half-dose PI therapy in STEMI. Eligible randomized, interventional, and observational studies reporting clinical outcomes were included. Pooled risk ratios were calculated using a random-effects model through pairwise meta-analysis and frequentist network meta-analysis (NMA) comparing short-term outcomes (≤ 30 days) among half-dose PI, full-dose PI, and PPCI.
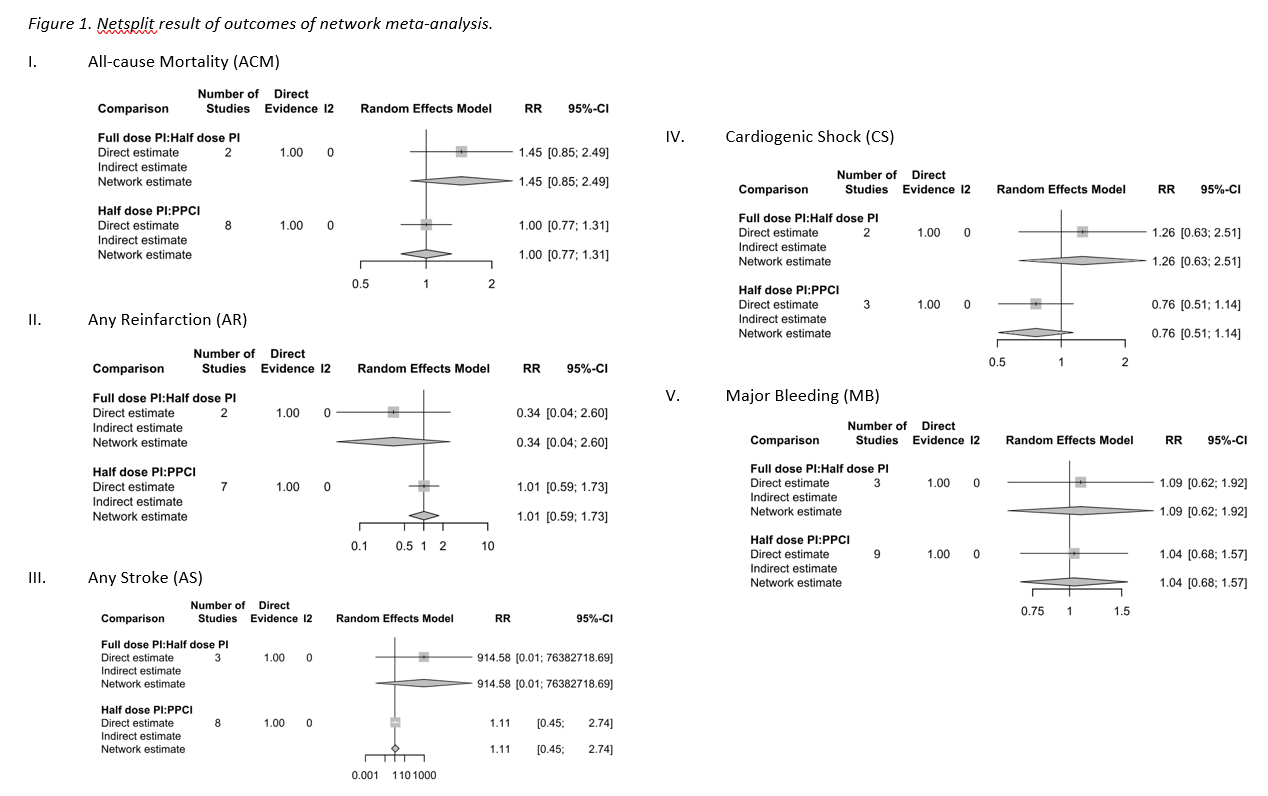
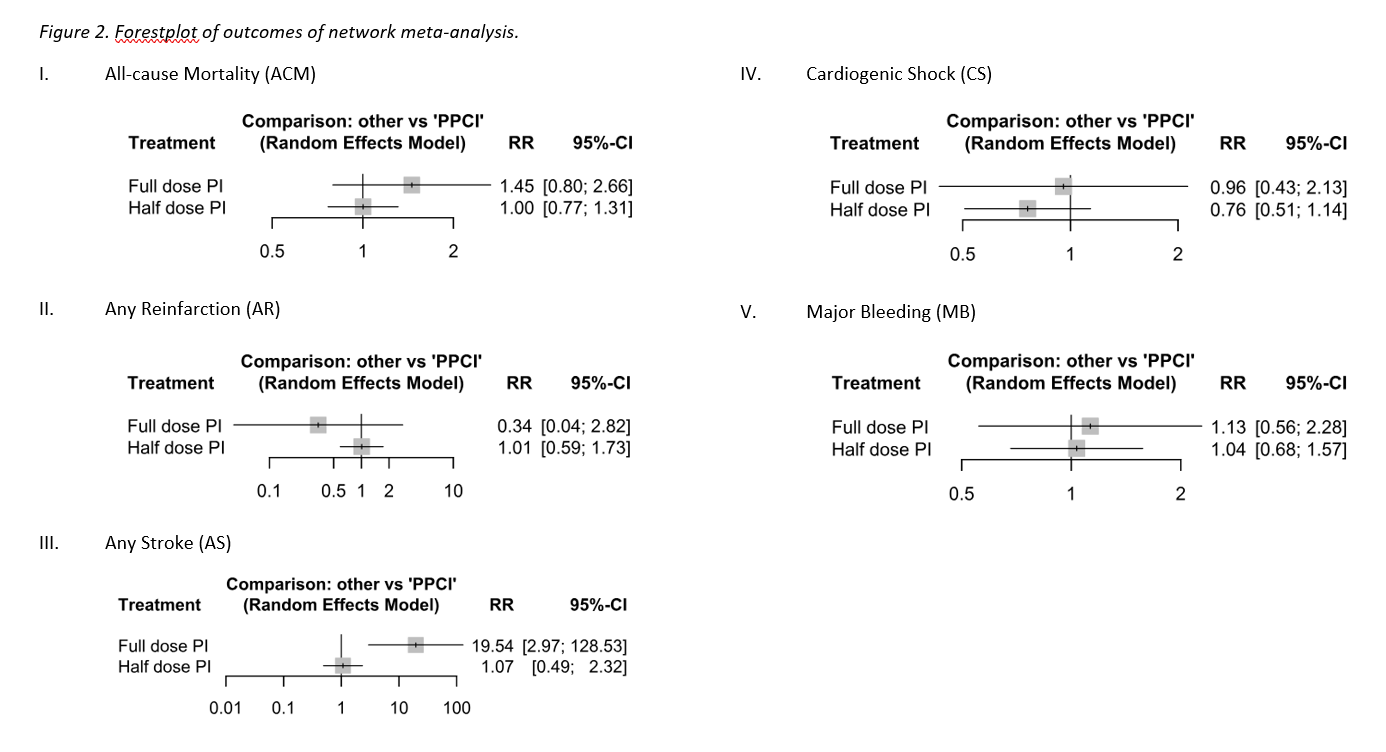
Results
Seventeen studies were included in the systematic review, of which eleven studies (n = 3,576) were analyzed quantitatively (half-dose PI = 1,917; PPCI = 1,480; full-dose PI = 179). Insignificant differences were observed across interventions in all-cause mortality, reinfarction, cardiogenic shock, and major bleeding (all p > 0.05), indicating comparable short-term efficacy and safety among the three reperfusion strategies. Half-dose PI and PPCI demonstrated comparable clinical outcomes across these endpoints, whereas stroke incidence was significantly higher with full-dose PI compared with PPCI (RR 19.54; 95 % CI 2.97 – 128.53; p = 0.002), while half-dose PI and PPCI exhibited comparable cerebrovascular safety (RR 1.07; 95 % CI 0.49 – 2.32; p = 0.8670). Ranking analysis identified half-dose PI as most favorable for mortality and hemodynamic stability (P-scores 0.7031 and 0.8264, respectively). Half-dose PI achieved earlier reperfusion (door-to-needle 30 - 60 minutes versus door-to-wire 90 - 120 minutes), minimizing ischemic delay in limited PCI settings.
Conclusion
Half-dose PI strategy offers short-term outcomes comparable to PPCI while avoiding the excess risk associated with full-dose PI. Half-dose PI enables earlier reperfusion with favorable efficacy and safety, representing a feasible alternative in settings with limited round-the-clock PCI access.