Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251109_0001
Prognostic Value of Global Longitudinal Strain, Holter Arrhythmias, and Biomarkers in Type 2 Diabetes After Myocardial Infarct: A Myanmar Cohort
By Swe Min Oo, Phway Mon Myo, Hein Zaw, Tun Naing Oo, Myint Zaw
Presenter
Swe Min Oo
Authors
Swe Min Oo1, Phway Mon Myo1, Hein Zaw1, Tun Naing Oo1, Myint Zaw2
Affiliation
700 Bedded Military Hospital , Myanmar1, Defence Services Medical Academy, Myanmar2
View Study Report
ABS20251109_0001
Clinical Trials & Science
Prognostic Value of Global Longitudinal Strain, Holter Arrhythmias, and Biomarkers in Type 2 Diabetes After Myocardial Infarct: A Myanmar Cohort
Swe Min Oo1, Phway Mon Myo1, Hein Zaw1, Tun Naing Oo1, Myint Zaw2
700 Bedded Military Hospital , Myanmar1, Defence Services Medical Academy, Myanmar2
Background
Background
Methods
We conducted a prospective, single-center cohortstudy at the 700 Bedded Military Hospital a tertiary care hospital in Pyin OoLwin, Myanmar. We enrolled 200 T2DM patients with LVEF >40% stabilized afteran acute MI. Pre-discharge, all patients underwent 2D speckle-trackingechocardiography for GLS, 24-hour Holter monitoring, and biomarker assessment(hs-cTnT, NT-pro BNP). The primary endpoint was 12-month MACE, a composite ofcardiovascular death, non-fatal recurrent MI, or non-fatal ischemic stroke.
Results
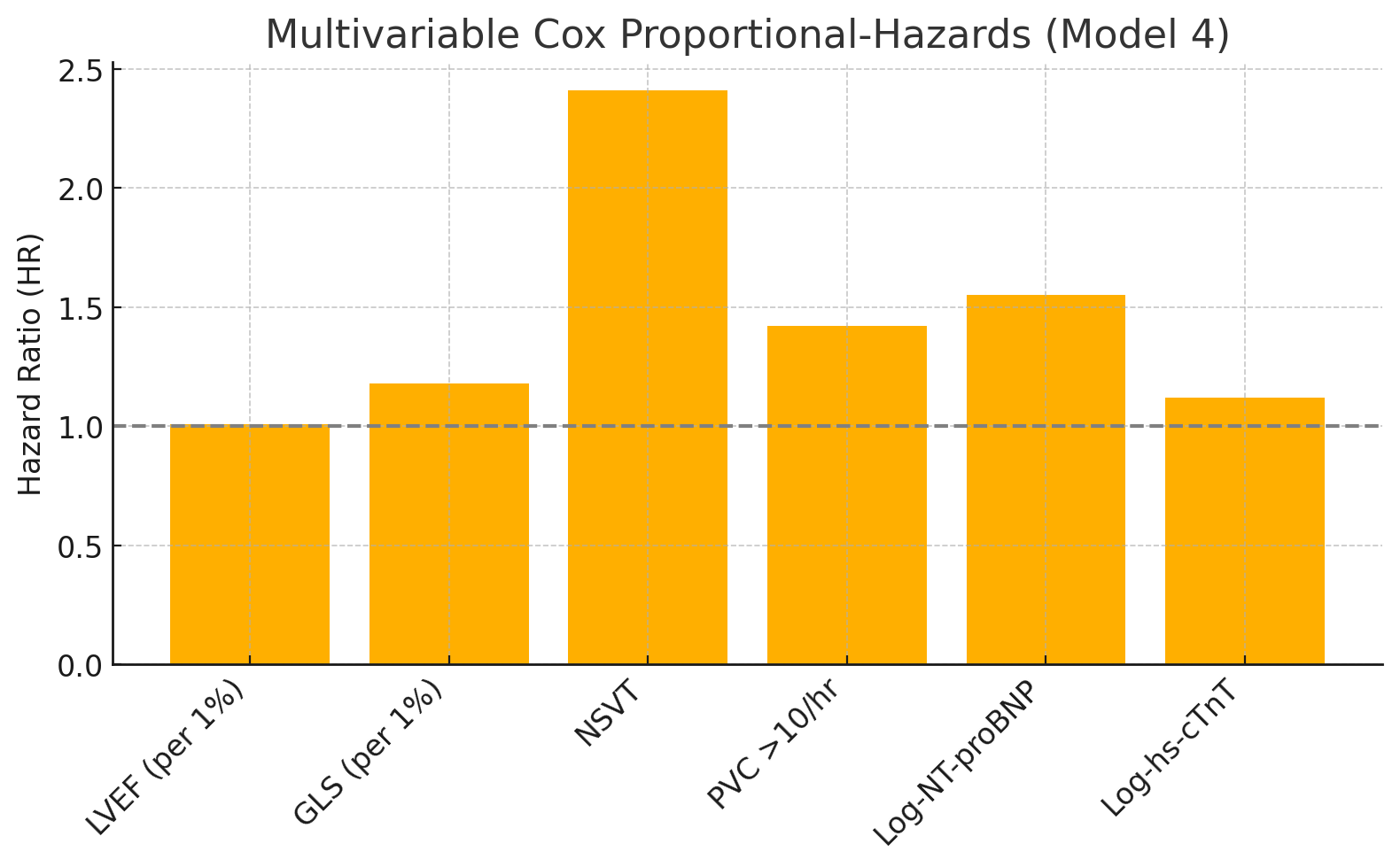
At 12 months, MACE occurred in 36 patients (18.0%). In an adjusted multivariable Cox regression model, impaired GLS (HR:1.18 per 1% worsening; 95% CI: 1.09-1.28), the presence of non-sustained ventricular tachycardia (NSVT) (HR: 2.41; 95% CI: 1.52-3.83), and log-transformed NT-pro BNP (HR: 1.55 per 1-SD increase; 95% CI: 1.24-1.93) were all significant, independent predictors of MACE (all p< 0.001). LVEF was not an independent predictor (p = 0.34). Adding this multi-marker panel to a base model (clinical factors + LVEF) significantly improved the C-statistic (from0.64 to 0.79; p < 0.01) and net reclassification (NRI: 0.38; p < 0.001). Full Model = Base + GLS + Holter + Biomarkers.C-Statistic = Concordance Statistic

Conclusion
In T2DM patients post-MI with relatively preserved LVEF, a multi-modality strategy integrating GLS, NSVT, and NT-pro BNP provides significant, independent, and incremental prognostic information over traditional risk factors. This approach identifies a high-risk cohort in Myanmar who may warrant more aggressive secondary prevention.