Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251107_0017
Intracoronary Alteplase as Bailout Therapy for High Thrombus Burden ST-Elevation Myocardial Infarction After Failed Aspiration Thrombectomy: A Case Series
By Kai Jie Phua, Jie Jun Wong
Presenter
Kai Jie Phua
Authors
Kai Jie Phua1, Jie Jun Wong2
Affiliation
National University of Singapore Yong Loo Lin School of Medicine, Singapore1, National Heart Centre Singapore, Singapore2
View Study Report
ABS20251107_0017
Pharmacotherapy (Coronary)
Intracoronary Alteplase as Bailout Therapy for High Thrombus Burden ST-Elevation Myocardial Infarction After Failed Aspiration Thrombectomy: A Case Series
Kai Jie Phua1, Jie Jun Wong2
National University of Singapore Yong Loo Lin School of Medicine, Singapore1, National Heart Centre Singapore, Singapore2
Background
High thrombotic burden in the coronary arteries during primary Percutaneous Coronary Intervention (PCI) for STEMI increases the risk of distal embolization, no-reflow, and suboptimal stent deployment, leading to worse clinical outcomes. Aspiration thrombectomy and glycoprotein IIb/IIIa inhibitors (GP2B/3Ai) are ways to reduce thrombus burden before stent implantation. However, aspiration thrombectomy has not shown a significant mortality benefit and is associated with increased stroke risk. While GP2b/3a inhibitors are bailout options for failed aspiration thrombectomy, they require prolonged infusion, which delays restoration of coronary flow and assessment of reperfusion, especially during STEMI PCI. Intracoronary low-dose thrombolytics provide a promising alternative, offering rapid, site-directed thrombus dissolution and facilitating aspiration. However, there are no standardized guidelines on the optimal dosage and administration of intracoronary thrombolytics available at present. We describe the safety and efficacy of intracoronary alteplase as bailout therapy following failed thrombectomy in high-thrombus burden STEMI.
Methods
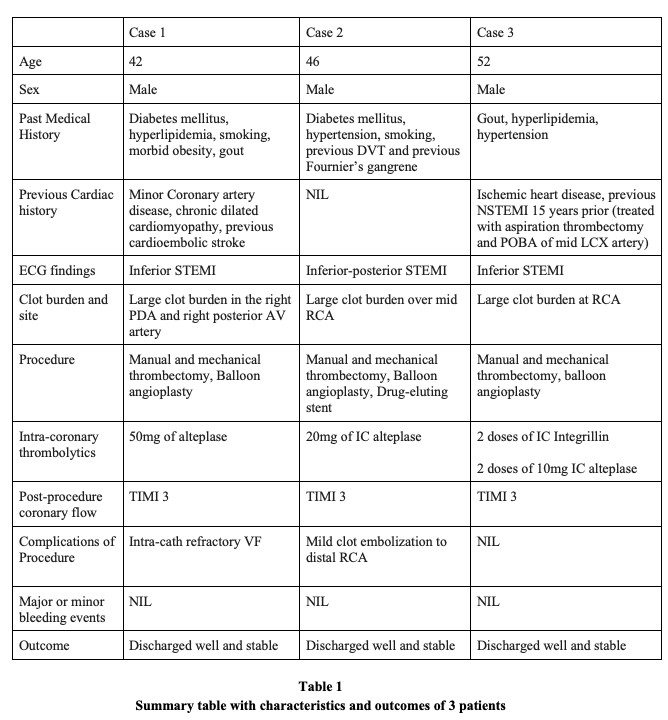
Three STEMI patients with angiographically confirmed large thrombus burden underwent primary PCI with dual-antiplatelet therapy (DAPT) and weight-adjusted unfractionated heparin (100 U/kg). Mechanical and/or manual aspiration thrombectomy was attempted but failed to restore adequate flow. Intracoronary alteplase (10–50 mg total) was delivered via aspiration or a microcatheter in fractional boluses, guided by angiographic response, followed by repeat aspiration and ballooning as indicated. Procedural success, TIMI flow, stent deployment, hemodynamic support requirements, and bleeding events were recorded.
Results
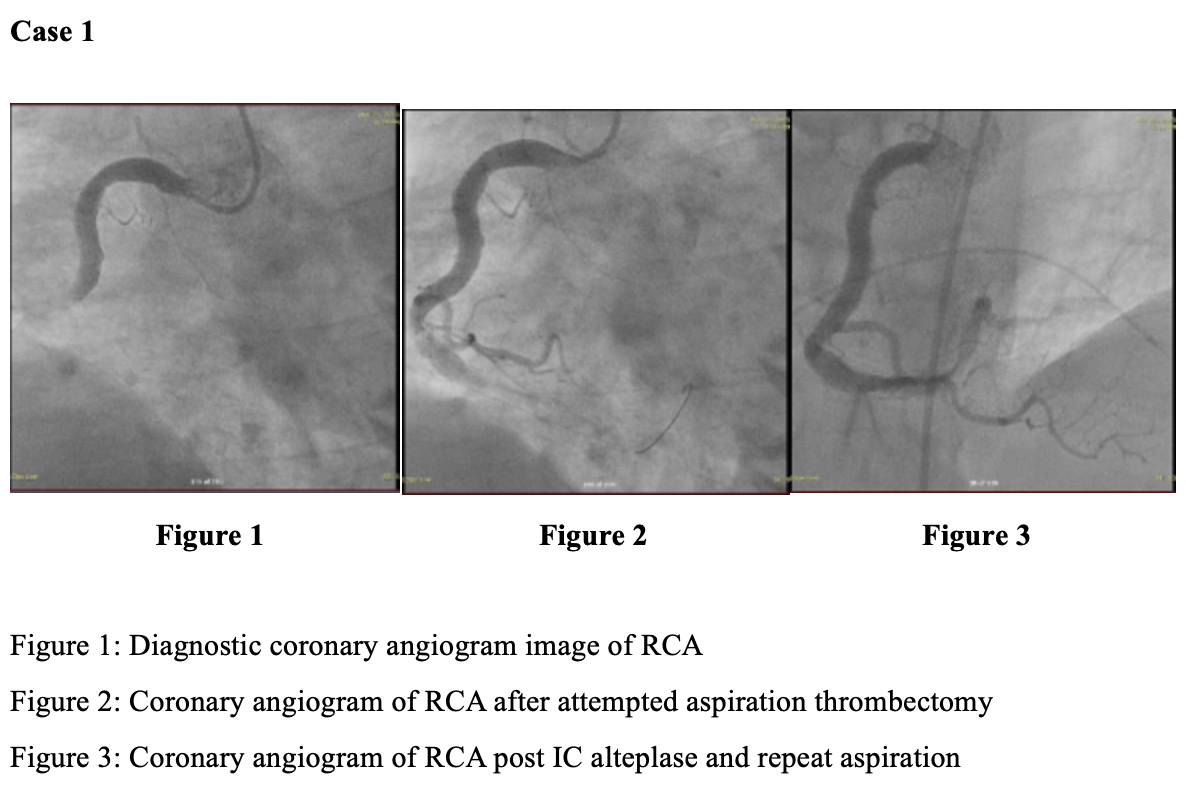
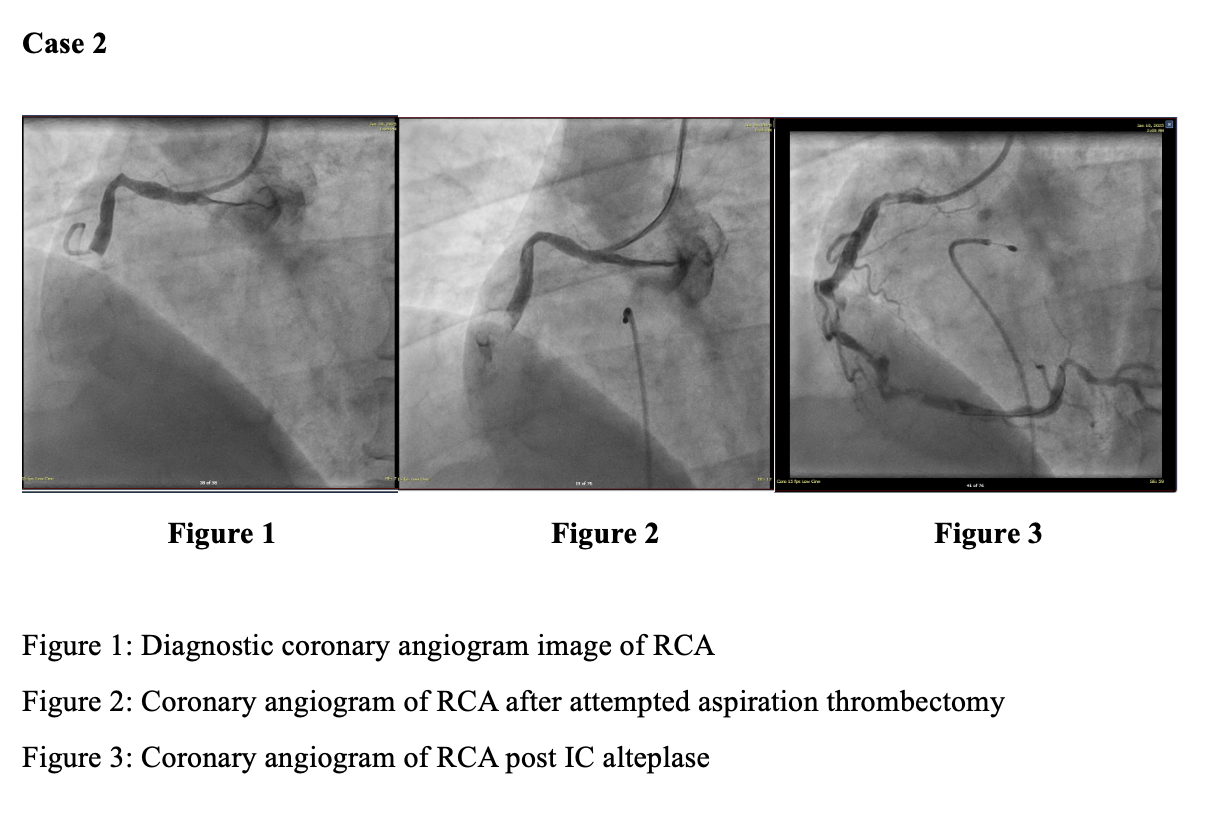
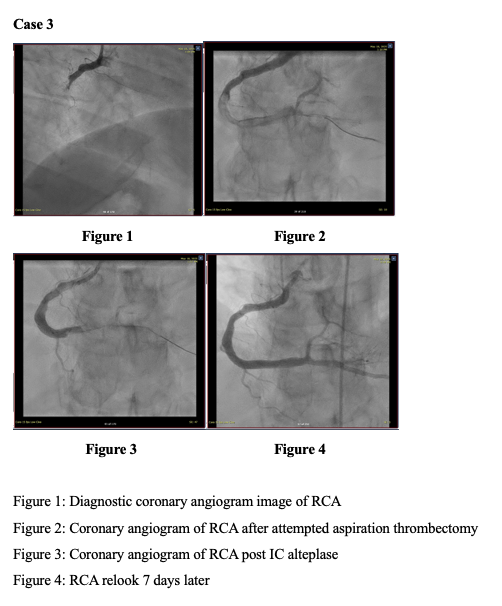
Intracoronary alteplase restored TIMI-3 flow in all three patients, enabling balloon angioplasty and, where indicated, definitive stent implantation. In Case 1, persistent thrombus despite manual and mechanical thrombectomy required 50 mg intracoronary alteplase, resulting in rapid clot dissolution. The patient experienced cardiogenic shock requiring VA-ECMO and IABP, with subsequent recovery of left ventricular function and successful device weaning. In Case 2, following failed aspiration, 20 mg alteplase enabled complete thrombus clearance and optimal stent deployment, with angiographic resolution confirmed on re-look imaging four days later. In Case 3, a persistent thrombus persisted despite aspiration and intracoronary GP2b/3ai. Still, the patient responded to 20 mg alteplase administered in staged boluses, achieving TIMI-3 flow with a marked reduction in clot burden. Across all cases, there were no major or minor bleeding events, access-site complications, or reinfarction. All patients were discharged hemodynamically stable.
Conclusion
In this real-world case series, catheter-directed intracoronary alteplase appears to be effective as bailout therapy for high-thrombus burden STEMI after failed aspiration thrombectomy and GP2A3B inhibition. Direct intracoronary fibrinolysis enabled successful reperfusion and PCI completion without bleeding complications. These findings support the selective use of targeted intracoronary thrombolysis in patients with large thrombus burden and low bleeding risk. Further larger studies are needed to affirm the use of intracoronary alteplase as a bailout therapy.