Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251107_0006
Stratifying Death Risk After Rotational Atherectomy Using the BCIS-CHIP Score
By Chin-Chin Chang, Yi-Lin Tsai, Wei-Ting Sung, Yu-Yu Lu, Shao-Sung Huang, Cheng-Hsueh Wu, Po-Hsun Huang, Tse-Ming Lu
Presenter
Chin-Chin Chang
Authors
Chin-Chin Chang1, Yi-Lin Tsai1, Wei-Ting Sung1, Yu-Yu Lu1, Shao-Sung Huang1, Cheng-Hsueh Wu1, Po-Hsun Huang1, Tse-Ming Lu1
Affiliation
Taipei Veterans General Hospital, Taiwan1
View Study Report
ABS20251107_0006
Calcified Lesion
Stratifying Death Risk After Rotational Atherectomy Using the BCIS-CHIP Score
Chin-Chin Chang1, Yi-Lin Tsai1, Wei-Ting Sung1, Yu-Yu Lu1, Shao-Sung Huang1, Cheng-Hsueh Wu1, Po-Hsun Huang1, Tse-Ming Lu1
Taipei Veterans General Hospital, Taiwan1
Background
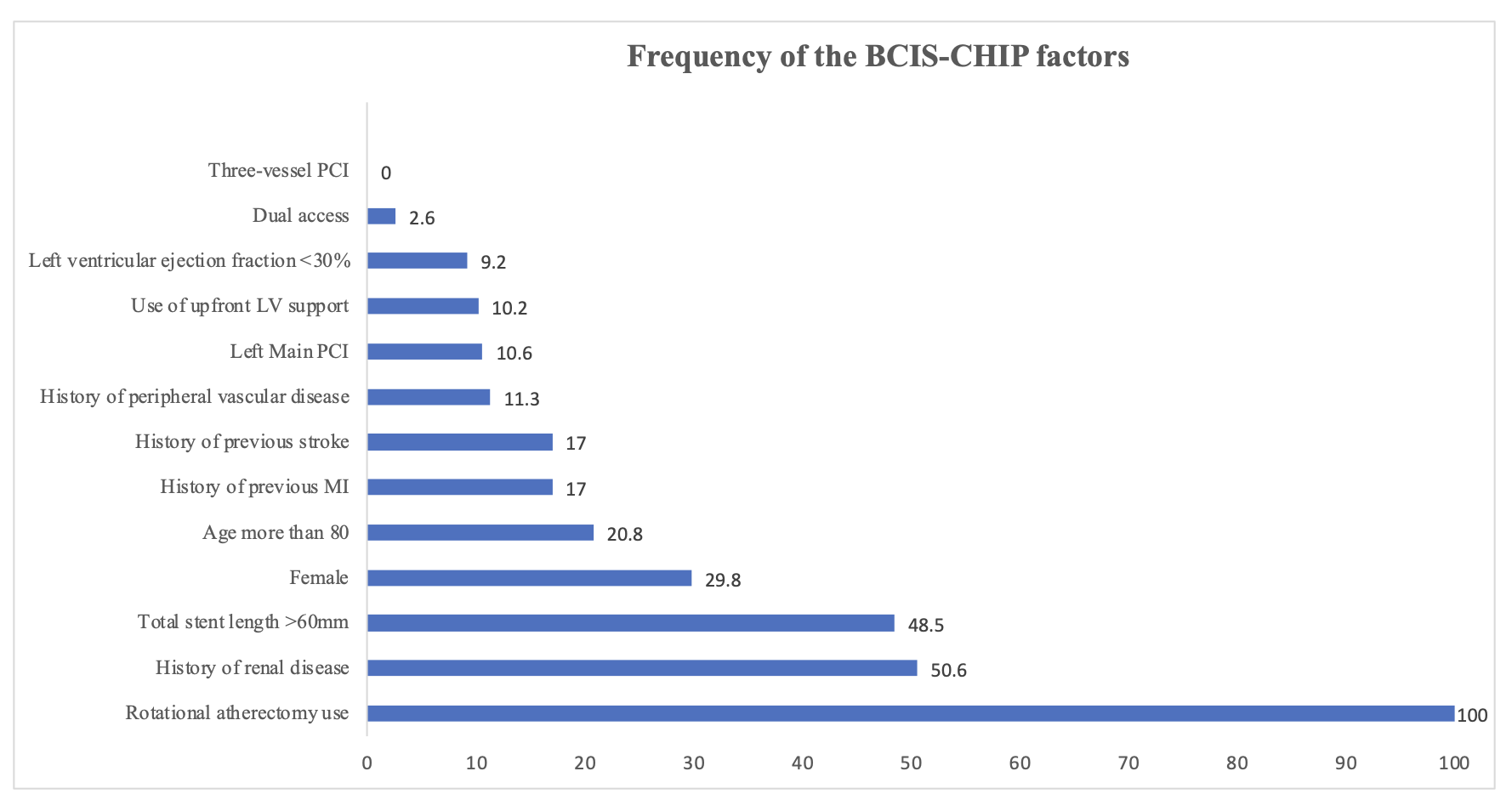
Patients undergoing rotational atherectomy (RA) for heavily calcified coronary artery disease (CAD) represent a complex and high-risk population. The British Cardiovascular Intervention Society–Complex High-Risk and Indicated Patients (BCIS-CHIP) score was developed to quantify procedural and clinical complexity, but its prognostic utility in RA-treated patients remains unclear.
Methods
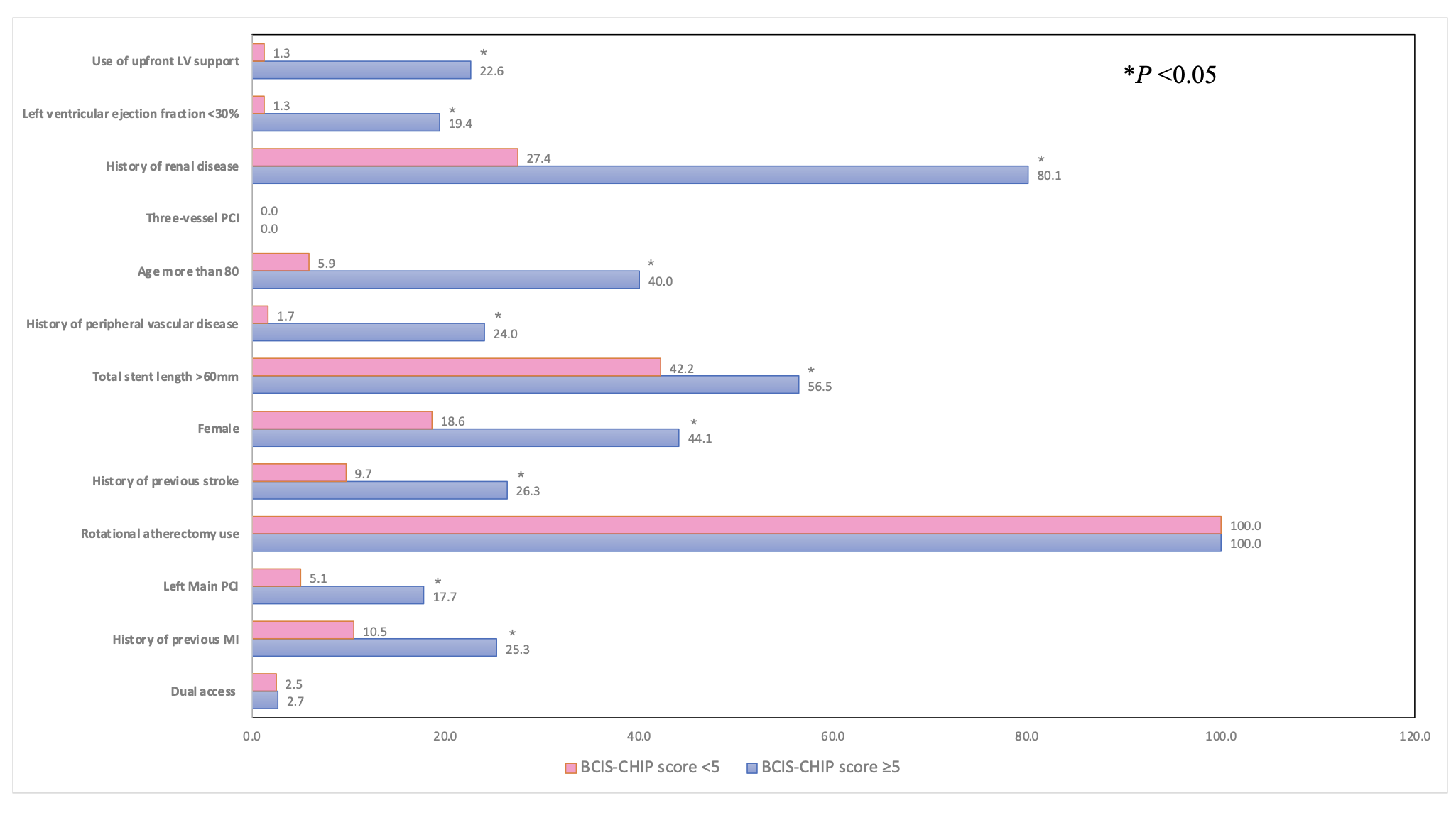
This retrospective, single-center study included consecutive patients with severe calcified CAD who underwent percutaneous coronary intervention (PCI) with RA between January 2017 and September 2024. The BCIS-CHIP score was calculated for each patient and used to stratify the cohort into a high-risk group (score ≥ 5) and a low-risk group (score < 5). Baseline characteristics, in-hospital outcomes, and long-term mortality were compared between groups. The association between the BCIS-CHIP score and all-cause mortality was evaluated using Cox proportional hazards models.
Results
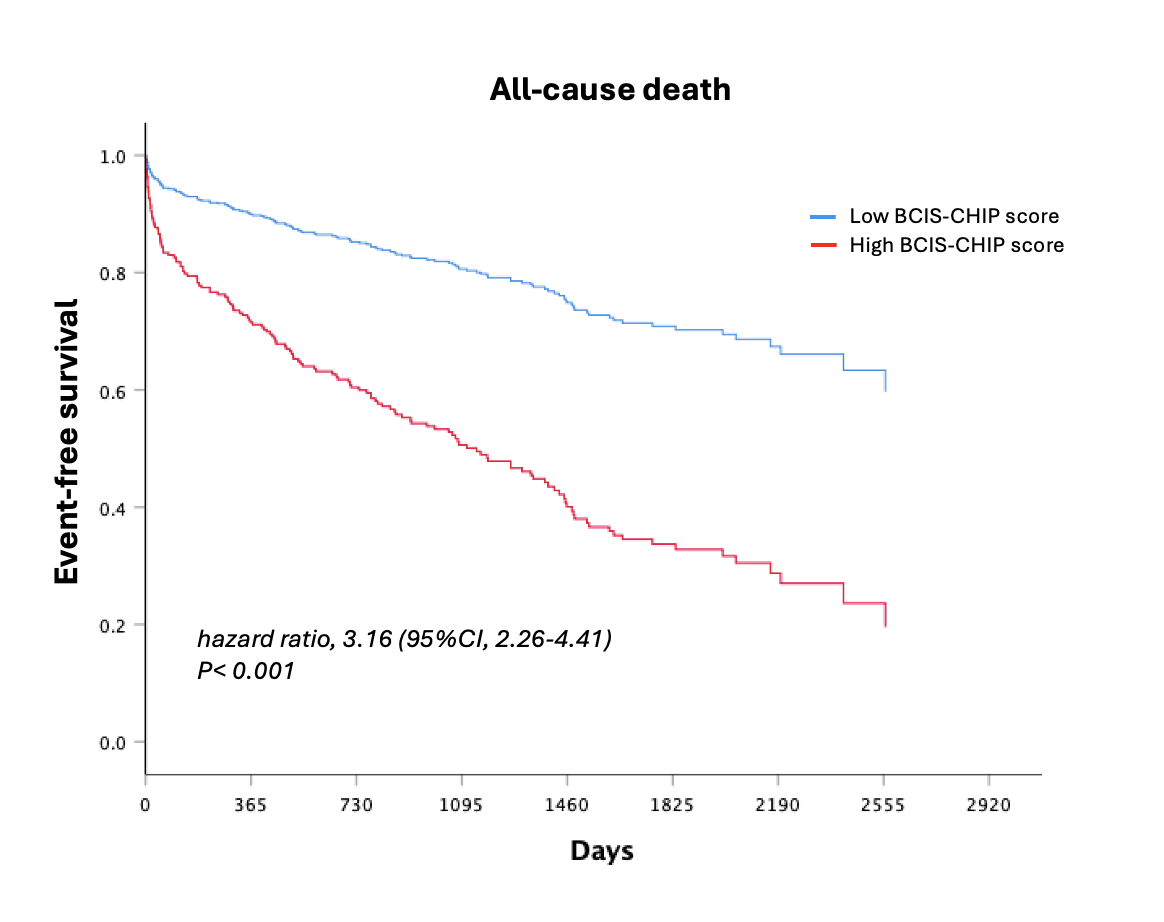
A total of 423 patients (mean age 70.8 ± 11.0 years, 70.8% men) were included. Patients with high BCIS-CHIP scores had significantly more comorbidities and procedural complexity compared with those with low scores. The in-hospital mortality rate was markedly higher in the high-risk group (16.7% vs. 1.7%; P < 0.001), as was 1-year mortality(26.3% vs. 4.6%; P < 0.001). Over a mean follow-up of 993 ± 762 days, a high BCIS-CHIP score was independently associated with increased all-cause mortality (hazard ratio 3.16; 95% CI 2.26–4.41; P < 0.001).
Conclusion
The BCIS-CHIP score effectively predicts all-cause mortality among patients with severe calcified CAD undergoing RA. This simple, validated risk tool may help clinicians identify high-risk patients who could benefit from intensified peri-procedural management and closer follow-up.