Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251107_0001
Patent Foramen Ovale Closure Following Cryptogenic Stroke or Transient Ischaemic Attack: An Extended Follow-Up of a Historical Cohort
By Siu Fung Wong, Mohamed Aboulesaad, Thomas Oswald, Timothy Bagnall, Christopher Broyd, James Cockburn, Joao Ferreira-Martins, Huda Abu-Own, David Hildick-Smith
Presenter
Siu Fung Wong
Authors
Siu Fung Wong1, Mohamed Aboulesaad1, Thomas Oswald1, Timothy Bagnall1, Christopher Broyd1, James Cockburn1, Joao Ferreira-Martins1, Huda Abu-Own2, David Hildick-Smith1
Affiliation
Royal Sussex County Hospital, United Kingdom1, Toronto General Hospital, Canada2
View Study Report
ABS20251107_0001
Other Structural Interventions
Patent Foramen Ovale Closure Following Cryptogenic Stroke or Transient Ischaemic Attack: An Extended Follow-Up of a Historical Cohort
Siu Fung Wong1, Mohamed Aboulesaad1, Thomas Oswald1, Timothy Bagnall1, Christopher Broyd1, James Cockburn1, Joao Ferreira-Martins1, Huda Abu-Own2, David Hildick-Smith1
Royal Sussex County Hospital, United Kingdom1, Toronto General Hospital, Canada2
Background
Patent foramen ovale (PFO) has been identified as a conduit for paradoxical embolism resulting in cryptogenic stroke or transient ischemic attack (TIA). Long-term data of PFO closure beyond 10 years have only been rarely reported, together with a poorly defined optimal post-closure antithrombotic treatment (AT) regimen. We aimed to evaluate the long-term efficacy and safety of closure beyond 10 years, and compare the efficacy of different duration of AT regimens among patients undergoing PFO closure for stroke or TIA at our unit.
Methods
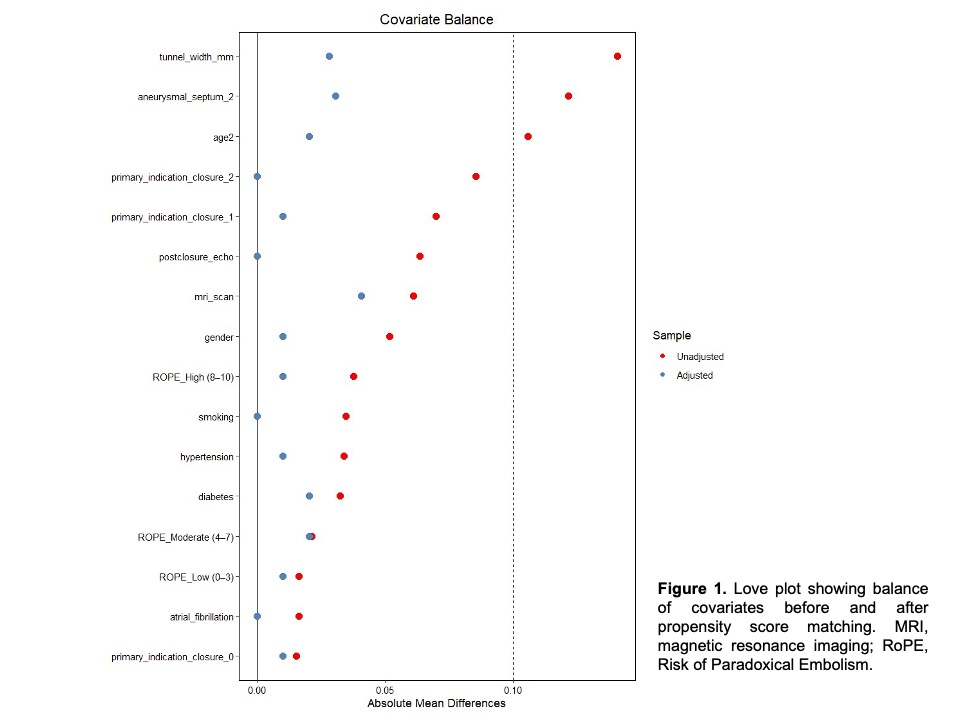
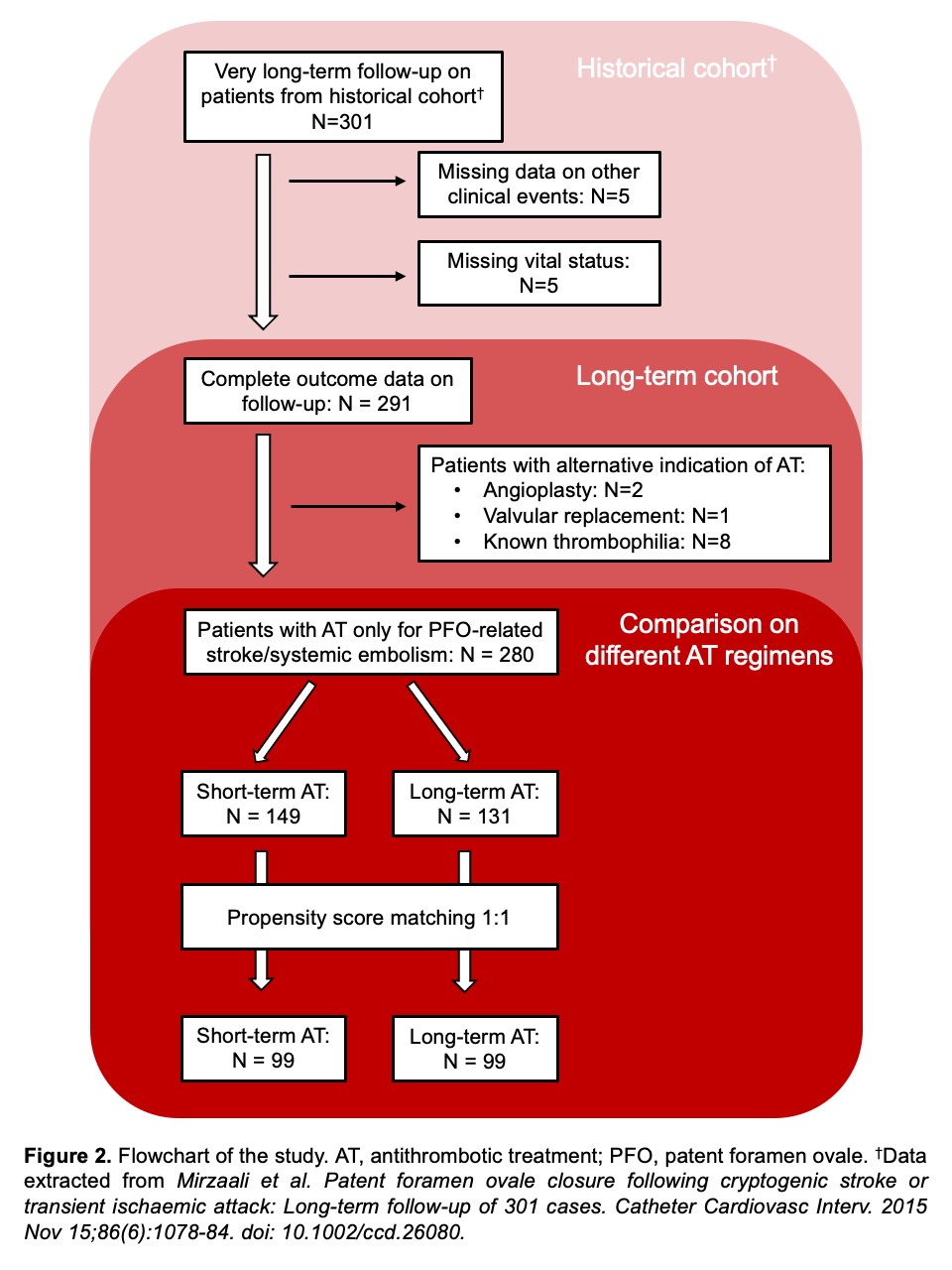
We reviewed the previously reported cohort of patient in a single centre who underwent PFO closure between May 2004 and January 2013. Outcomes including recurrent stroke or TIA, bleeding, major bleeding, venous thromboembolism (VTE), newly diagnosed atrial fibrillation (AF) and all-cause death were adjudicated. The entire cohort was further stratified into short- and long-term antithrombotic treatment (AT) groups based on the duration of post-procedural AT. Propensity score matching was performed to adjust for difference in baseline characteristics across subgroups (Figure 1). The same set of outcomes is compared between subgroups before and after adjustment for variables. Figure 2 summarized a flowchart of the study.
Results
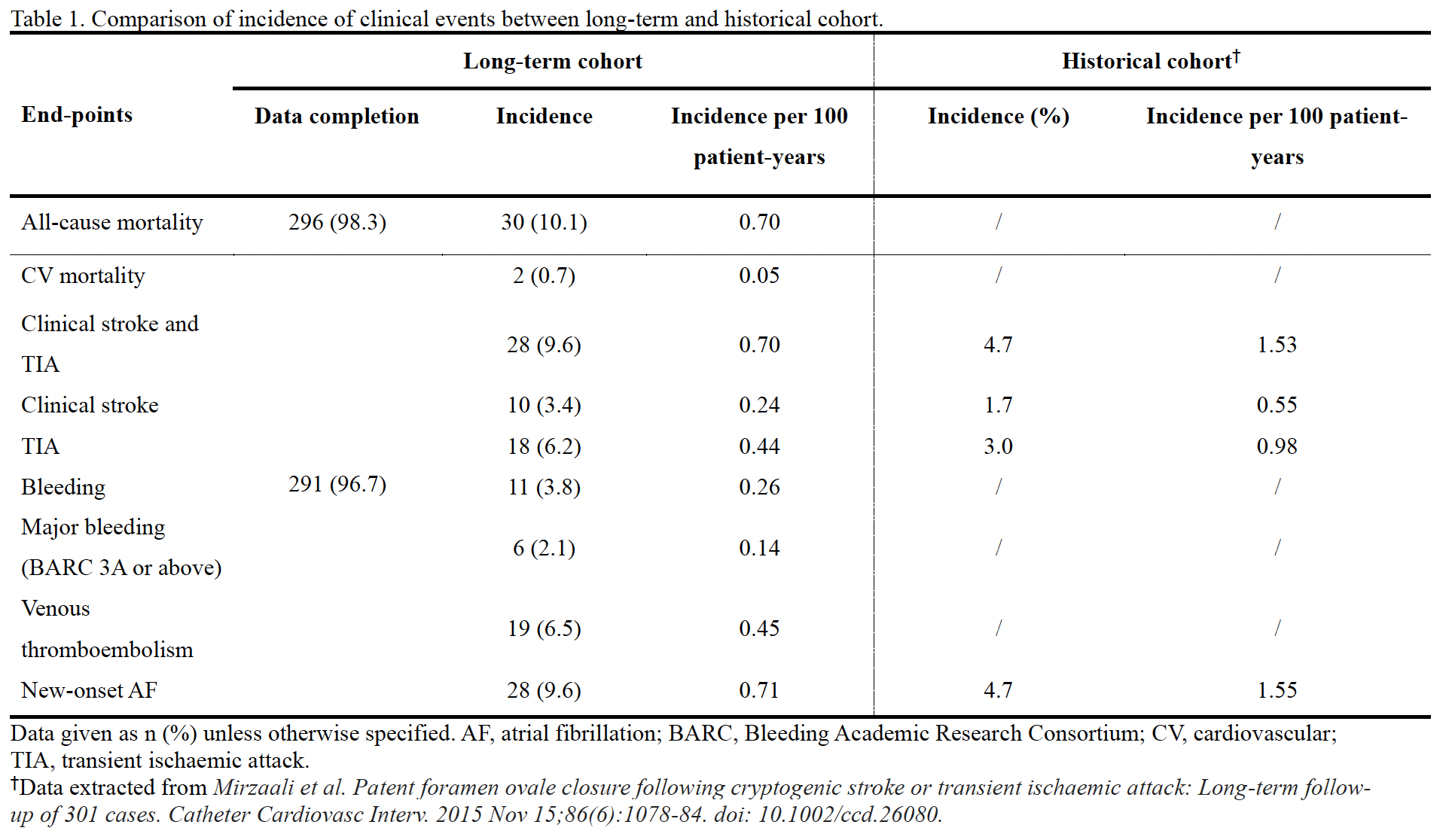
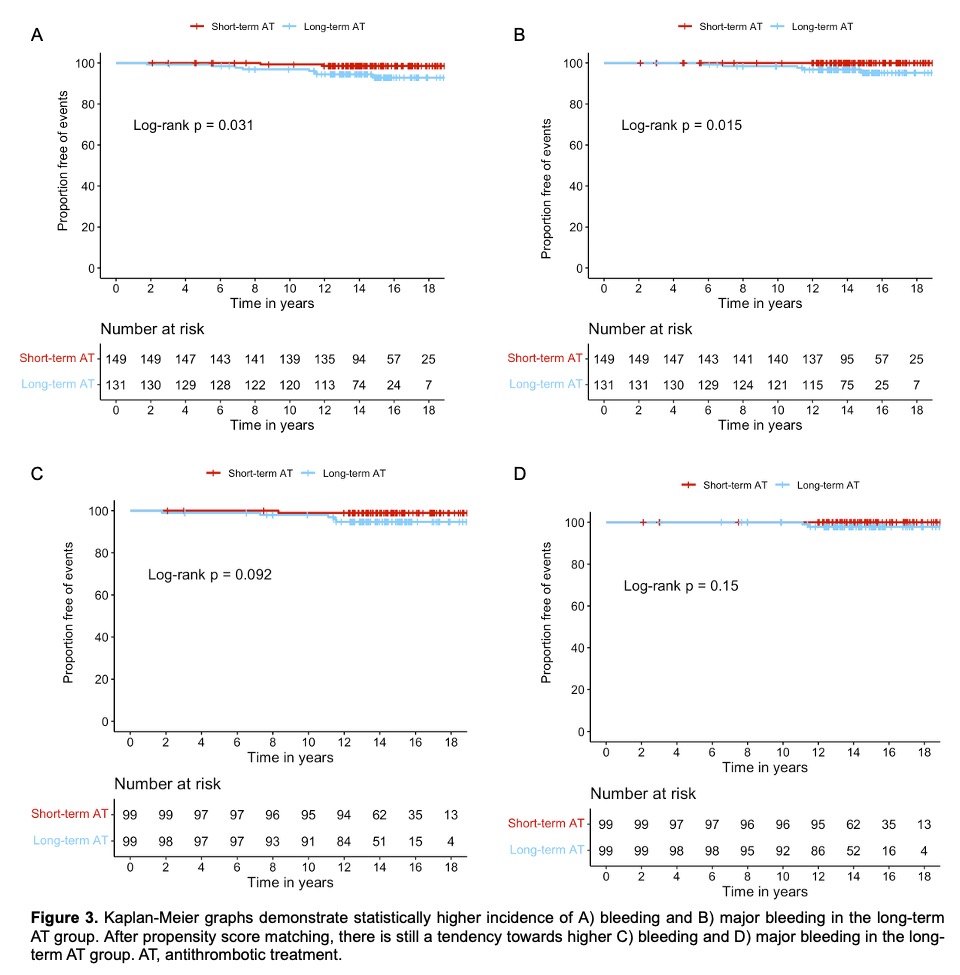
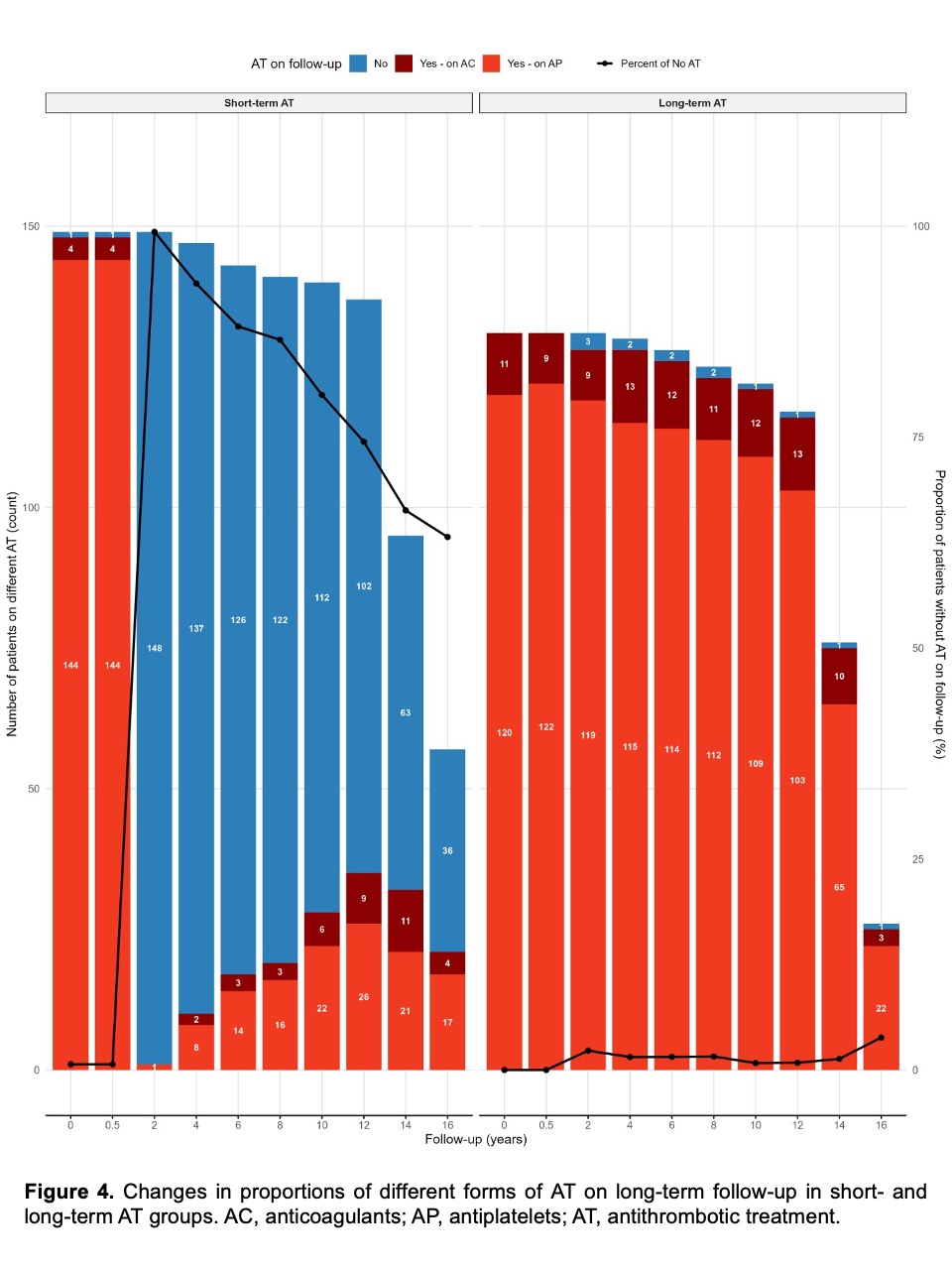
301 patients were included in the analysis. Median follow-up duration was 15.0 [95% confidence interval (CI) 14.7-15.3] years. Follow-up was complete in 296 (98.3%) patients for mortality and in 291 (96.7%) patients for stroke and TIA, bleeding, major bleeding, VTE and newly diagnosed AF. Recurrent stroke and TIA were observed in 28 patients (0.70 per 100 patient-years). Bleeding, major bleeding and VTE occurred in 11 (0.26 per 100 patient-years), 6 (0.14 per 100 patient-years) and 19 patients (0.45 per 100 patient-years) respectively. 28 patients (0.71 per 100 patient-years) were diagnosed to have atrial fibrillation. 30 patients (0.70 per 100 patient-years) died (Table 1). Patients receiving long-term AT experienced more bleeding and major bleeding events (log-rank p=0.03 and 0.02 respectively), and had a tendency towards more frequent bleeding (long-rank p=0.09) after propensity score matching (Figures 3A-D). All the other outcome events are similar between subgroups. 59.2% of patients in the short-term AT group remained free of AT by the end of the study period (Figure 4).
Conclusion
Benefits from PFO closure may extend into longer term given the persistently low incidence of adverse clinical outcomes in the long run after procedure. A limited post-closure AT regimen is equally effective in prevention of recurrent embolic events in the long run whilst associated with potentially less bleeding.