Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251106_0013
Imaging of Vulnerable Plaques in Coronary Artery Disease: A Clinical Experience
By Rohit Mody
Presenter
Rohit Mody
Authors
Rohit Mody1
Affiliation
Mody Harvard Cardiac Institute & Research Centre , India1
View Study Report
ABS20251106_0013
Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Imaging of Vulnerable Plaques in Coronary Artery Disease: A Clinical Experience
Rohit Mody1
Mody Harvard Cardiac Institute & Research Centre , India1
Background
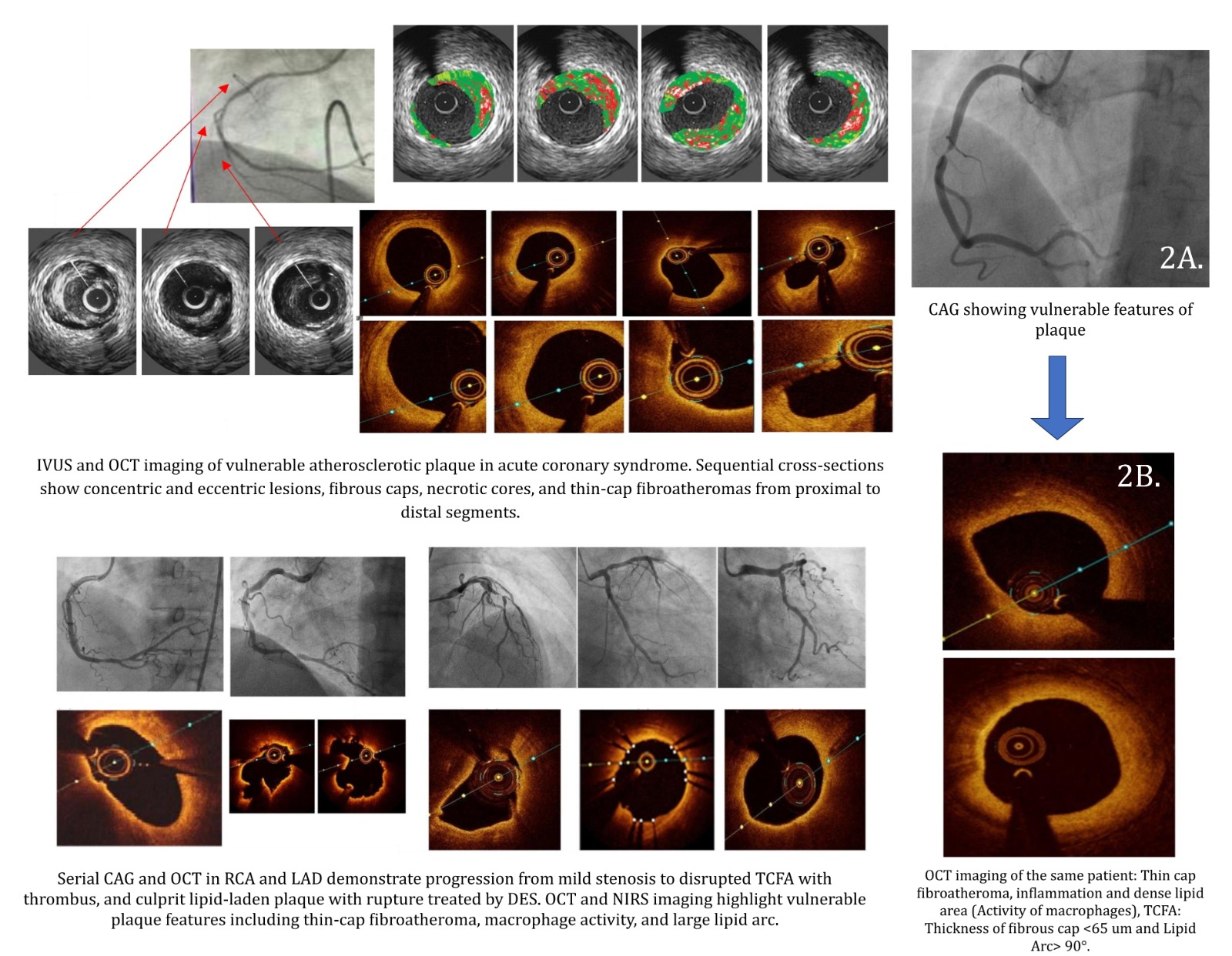
Acute coronary syndromes (ACS) are most frequentlyprecipitated by disruption of vulnerable plaques, typically thin-capfibroatheromas (TCFAs) with large necrotic cores, macrophage infiltration, andpositive remodeling. Traditional coronary angiography, while essential forlumen visualization, fails to provide detailed insight into plaque compositionor vulnerability.
Methods
A prospective observational registry was conducted at ModyHarvard Cardiac Institute between March 2023 and June 2024. Patients undergoingcoronary angiography for stable angina or ACS in whom intravascular imaging wasperformed were included.
- Age ≥18 years.
- Undergoing PCI or diagnostic angiography where imaging (OCT, IVUS, or NIRS-IVUS) was performed.
- Presence of at least one angiographically intermediate or non-culprit lesion.
- Cardiogenic shock.
- Chronic total occlusion lesions not amenable to imaging.
- Contraindications to intracoronary imaging catheters (e.g., very small vessels <2 mm).
- OCT: Used to identify thin fibrous caps (<65 μm), lipid arc >180°, macrophage clusters, and microchannels.
- IVUS/NIRS: Used for plaque burden (>70%), remodeling index, and lipid-core burden index (max LCBI over 4 mm ≥400 considered high-risk).
- Imaging was performed in both culprit and non-culprit segments where feasible.
- Primary Endpoint: Prevalence of vulnerable plaque features in the study population.
- Secondary Endpoints: Association between imaging-defined vulnerability and clinical outcomes at 12 months (MACE: death, MI, unplanned revascularization).
Results
Baseline Characteristics
- OCT (n=80 lesions):
- Thin-cap fibroatheromas (cap thickness <65 μm) were identified in 22% of lesions.
- Macrophage accumulation was present in 30%.
- Microchannels suggestive of neovascularization were seen in 12%.
- Plaque rupture was detected in 14% of ACS culprit lesions.
- NIRS-IVUS (n=70 lesions):
- Mean plaque burden was 69 ± 8%.
- Positive remodeling (remodeling index >1.05) in 18%.
- High-risk LCBI ≥400 was present in 21%.
- Lesions with high LCBI were more frequent in diabetic patients (p=0.01).
- Combined Risk Features:
- 16% of lesions met ≥3 high-risk imaging criteria (thin fibrous cap, large lipid core, high plaque burden, positive remodeling).
- Non-culprit lesions with these features were often angiographically mild-to-moderate (40–60% stenosis).
- Imaging changed management in 28% of cases:
- Additional stenting or lesion preparation in calcified plaques.
- Deferral of angiographically “significant” lesions lacking vulnerability features.
- Intensification of medical therapy (high-intensity statins, PCSK9 inhibitors) for patients with multiple vulnerable plaques.
- Overall MACE occurred in 9% of patients.
- Patients with at least one high-risk plaque (≥3 features or LCBI ≥400) had significantly higher MACE (17% vs 4%, p=0.02).
- Non-culprit lesion–related events occurred in 5 patients, all of whom had baseline vulnerable plaque characteristics.
Conclusion
In this real-world Indian registry, intravascular imagingidentified a high prevalence of vulnerable plaques, particularly among diabeticand younger patients. Imaging-defined vulnerability was associated withsignificantly higher adverse event rates at one year. These findings underscorethe need for routine integration of imaging in risk stratification andmanagement of CAD in Indian practice. Larger studies are warranted to determinewhether pre-emptive interventions in high-risk plaques can improve outcomes inthis unique population.
This registry provides novel insights into the prevalenceand prognostic value of vulnerable plaque imaging in Indian patients. Severalkey findings deserve emphasis:
This registry provides novel insights into the prevalenceand prognostic value of vulnerable plaque imaging in Indian patients. Severalkey findings deserve emphasis:
- High Prevalence of Vulnerable Plaques in Indian Patients
Nearly one in five imaged lesions demonstrated TCFA, and 21% had high LCBI by NIRS. This rate is comparable to international cohorts but appears amplified by the younger age and higher prevalence of diabetes in our population. - Angiographic Underestimation
A significant proportion of angiographically “non-significant” lesions harbored vulnerable plaque features, reinforcing the limitations of angiography alone in risk stratification. This highlights the importance of physiology and imaging integration. - Management Impact
Imaging altered procedural decisions in over one-quarter of cases, reflecting its utility not only in identifying risk but also in guiding PCI optimization and medical management. For example, lesions without vulnerability features could safely be deferred, potentially reducing unnecessary interventions. - Prognostic Significance
Patients with vulnerable plaque features had a 4-fold higher risk of MACE at 12 months. This parallels findings from PROSPECT, CLIMA, and other large registries, and suggests that imaging-defined vulnerability can meaningfully stratify risk in Indian patients as well.