Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251106_0010
Intervention for Chronic Total Occlusion Involving Bifurcation Lesions: Insights From the TRIO CTO (Taiwan Research Initiative on Coronary Total Occlusion) Registry
By Ying-Chang Tung
Presenter
Ying-Chang Tung
Authors
Ying-Chang Tung1
Affiliation
Linkou Chang Gung Memorial Hospital, Taiwan1
View Study Report
ABS20251106_0010
CTO
Intervention for Chronic Total Occlusion Involving Bifurcation Lesions: Insights From the TRIO CTO (Taiwan Research Initiative on Coronary Total Occlusion) Registry
Ying-Chang Tung1
Linkou Chang Gung Memorial Hospital, Taiwan1
Background
Percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) remains technically challenging, with lower success and higher complication rates than non-CTO PCI. Among lesion-specific factors, bifurcation involvement within or near the occluded segment adds substantial procedural complexity. Approximately one-third of CTOs contain a relevant side branch (SB), increasing the risk of dissection, SB occlusion, or subintimal shift.
Methods
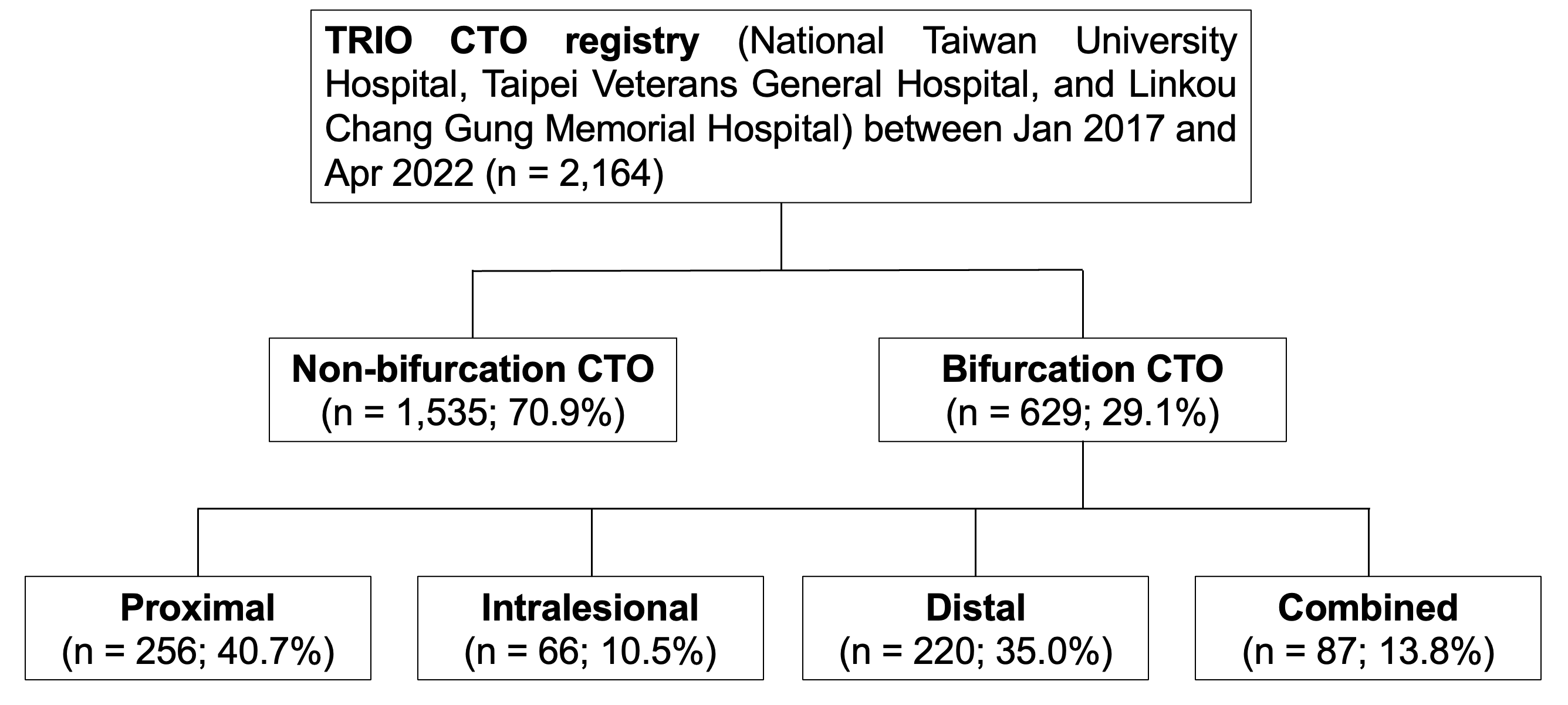
We retrospectively analyzed CTO PCI procedures performed between January 2017 and April 2022 in the TRIO-CTO registry, a collaborative study among three tertiary centers in northern Taiwan: National Taiwan University Hospital, Taipei Veterans General Hospital, and Linkou Chang Gung Memorial Hospital.
Results
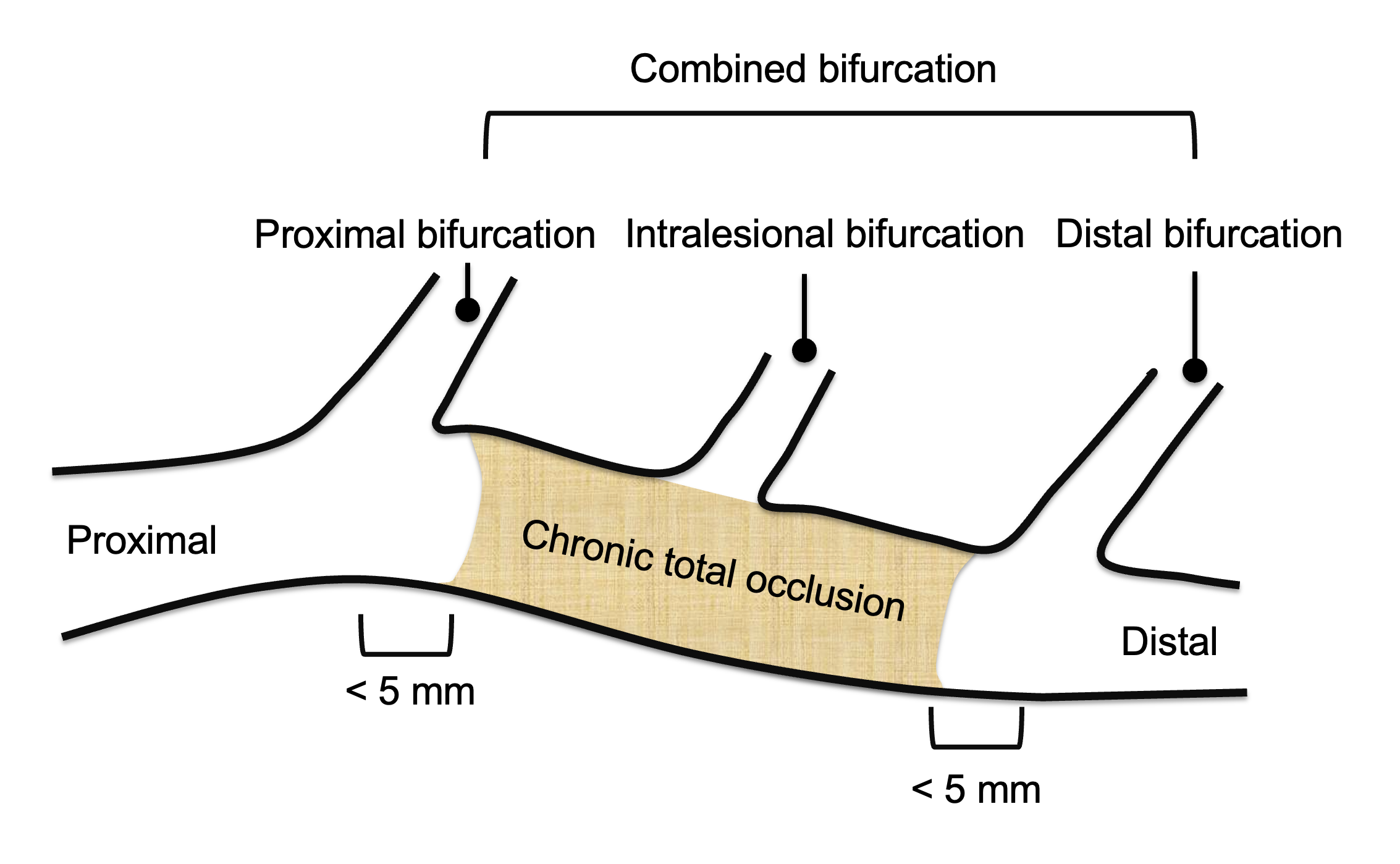
A total of 2,164 CTO PCI procedures were analyzed between January 2017 and April 2022, of which 29.1% were classified as bifurcation CTO. Among these, 40.7% involved the proximal cap, 35.0% the distal cap, 10.5% were intralesional, and 13.0% were combined bifurcations.
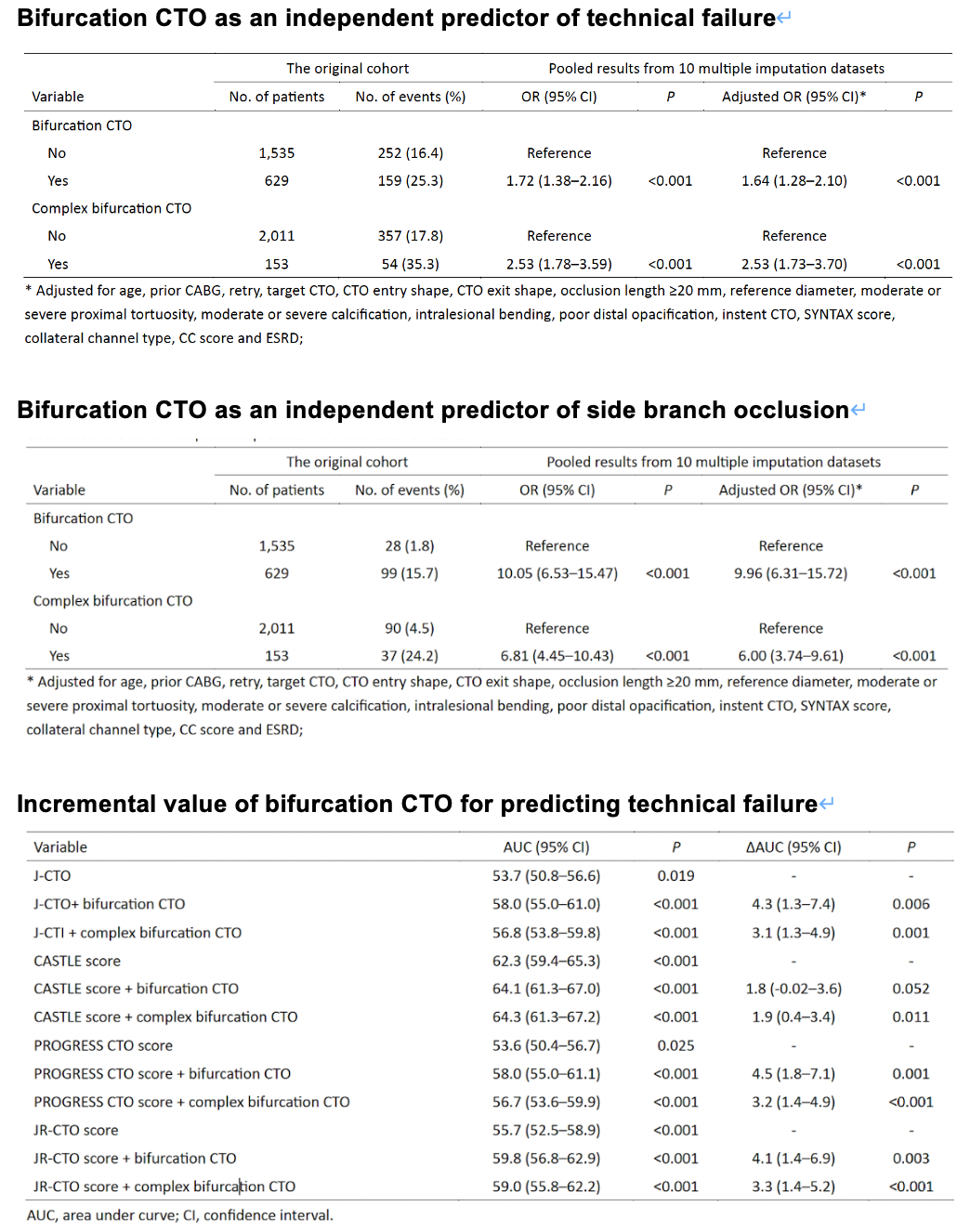
Conclusion
Bifurcation involvement is common in CTO PCI and independently predicts technical failure, primarily due to a higher risk of side-branch occlusion. Complex bifurcation CTOs, particularly intralesional and combined types, are associated with the lowest procedural success. Incorporating bifurcation characteristics into existing CTO scoring systems significantly improves the prediction of technical outcomes and may enhance procedural planning and risk stratification.