Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251103_0007
Impact of Reimbursement Policy on Outcomes of Transcatheter Aortic Valve Replacement in Taiwan: A Nationwide Quasi-Experimental Study (2013–2021)
By Wei-Hsian Yin, Huang-Chiu Lin, Chia-Hui (Elise) Tan
Presenter
Chia-Hui (Elise) Tan
Authors
Wei-Hsian Yin1, Huang-Chiu Lin1, Chia-Hui (Elise) Tan2
Affiliation
Heart Center, Cheng-Hsin General Hospital and School of Medicine, National Yang Ming Chiao Tung Univ, Taiwan1, Department of Health Service Administration, China Medical University, Taiwan2
View Study Report
ABS20251103_0007
Minimalist TAVR
Impact of Reimbursement Policy on Outcomes of Transcatheter Aortic Valve Replacement in Taiwan: A Nationwide Quasi-Experimental Study (2013–2021)
Wei-Hsian Yin1, Huang-Chiu Lin1, Chia-Hui (Elise) Tan2
Heart Center, Cheng-Hsin General Hospital and School of Medicine, National Yang Ming Chiao Tung Univ, Taiwan1, Department of Health Service Administration, China Medical University, Taiwan2
Background
Transcatheter aortic valve replacement (TAVR), which was first performed in 2002, offers a less-invasive alternative to SAVR, avoiding the need for a sternotomy and cardiopulmonary bypass by delivering a bioprosthetic valve via a catheter. Pivotal early trials demonstrated the transformative potential of TAVR, showing a significant reduction in mortality for inoperable patients and non-inferiority to SAVR in high-risk cohorts. TAVR also appears to be an alternative for severe AS patients with high or even intermediate operative risk. Better survival outcomes of the procedures were shown in numerous randomized controlled trials.
Methods
This was a quasi-experimental study that used the nationwide claims data, including admission, outpatient, and prescription records from 2012 to 2021, and linked it to the Cause of Death data via scrambled identification. Patients who underwent TAVR between January 1, 2013, and December 31, 2021, and had the primary or secondary diagnosis of severe aortic stenosis (AS) were included. Patients who received TAVR were defined as the index date and followed until event occurrence, death, or the end of the study period (December 31, 2021), whichever came first. Then, patients were divided into three groups via the date of the received procedure (2013-2016, 2017-2020, and 2021-).
Results
Among 1,161 TAVR patients (mean age 81.8 years; 53.9% female), 30-day mortality remained stable (4.4%), while vascular complications declined over time (5.6% → 2.2%). After adjusting for baseline characteristics, the results showed reimbursement expansion did not affect 30-day mortality but was associated with improved long-term outcomes (Table 1). Compared with the out-of-pocket period, the partial reimbursement strategy significantly reduced the risk of ACM (HR 0.75, 95% CI 0.59–0.95) and PPI (HR 0.56, 95% CI 0.41–0.76) (Table 2).
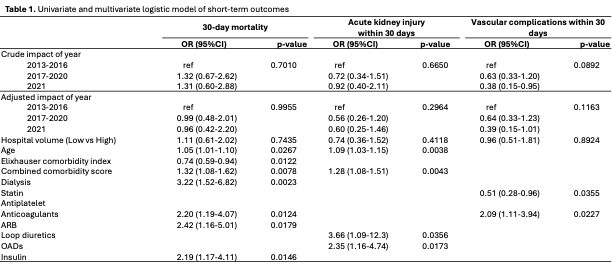
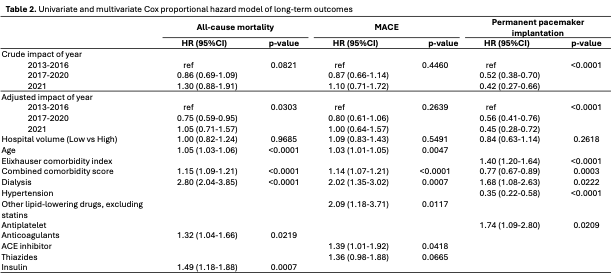
Conclusion
Progressive expansion of TAVR reimbursement of health insurance coverage improved long-term survival and reduced device-related complications without compromising short-term safety, highlighting the positive impact of equitable financial access on procedural outcomes.