Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251030_0001
Elevated Plasma Homocysteine Predicts Long-Term Adverse Cardiovascular Outcomes After Percutaneous Coronary Intervention
By Sue-Ping Chang, Jien-Jiun Chen, Pang-Shuo Huang
Presenter
Sue-Ping Chang
Authors
Sue-Ping Chang1, Jien-Jiun Chen2, Pang-Shuo Huang3
Affiliation
National Taiwan University Hospital Yunlin Branch, Taiwan1, Taichung Municipal Senior Rehabilitation Hospital, Taiwan2, Fu Jen Catholic University Hospital, Taiwan3
View Study Report
ABS20251030_0001
Clinical Trials & Science
Elevated Plasma Homocysteine Predicts Long-Term Adverse Cardiovascular Outcomes After Percutaneous Coronary Intervention
Sue-Ping Chang1, Jien-Jiun Chen2, Pang-Shuo Huang3
National Taiwan University Hospital Yunlin Branch, Taiwan1, Taichung Municipal Senior Rehabilitation Hospital, Taiwan2, Fu Jen Catholic University Hospital, Taiwan3
Background
Elevated plasma homocysteine is associated with increased cardiovascular risk and adverse outcomes after percutaneous coronary intervention (PCI). Its long-term prognostic value in the drug-eluting stent (DES) era remains unclear.
Methods
We retrospectively analyzed 954 patients who underwent PCI with stent implantation for acute coronary syndrome or refractory angina between August 2006 and September 2024 at National Taiwan University Hospital, Yunlin Branch, Taiwan. Patients receiving venous graft interventions were excluded. Baseline plasma homocysteine levels were stratified into quartiles. The primary endpoint was major adverse cardiovascular events (MACE), defined as a composite of all-cause death, nonfatal myocardial infarction (MI), ischemic stroke, and target lesion revascularization (TLR). Secondary endpoints included non-TLR, heart failure hospitalization (HFH), and arrhythmic events (ventricular arrhythmias or new-onset atrial fibrillation). Event-free survival was assessed using Kaplan–Meier analysis. Multivariable Cox proportional hazards models adjusted for conventional risk factors were used to estimate hazard ratios (HRs) with 95% confidence intervals (CIs).
Results
During a mean follow-up of 53.0 ± 39.5 months, 130 patients (13.3%) experienced MACE, including 7 deaths (0.7%), 14 nonfatal MI (1.5%), 20 ischemic strokes (2.1%), and 98 TLRs (10.3%). Secondary events included non-TLR in 263 patients (27.6%), HFH in 40 (4.2%), and arrhythmic events in 17 (1.8%). MACE incidence increased progressively across homocysteine quartiles (p < 0.001). Compared with the lowest quartile, the highest quartile had a significantly higher risk of MACE (adjusted HR: 2.46; 95% CI: 1.32–4.59; p = 0.005). Elevated homocysteine independently predicted all-cause death (p = 0.039), TLR (p = 0.006), non-TLR (p = 0.017), and HFH (p = 0.005), but not nonfatal MI (p = 0.706), ischemic stroke (p = 0.114), or arrhythmic events (p = 0.556).
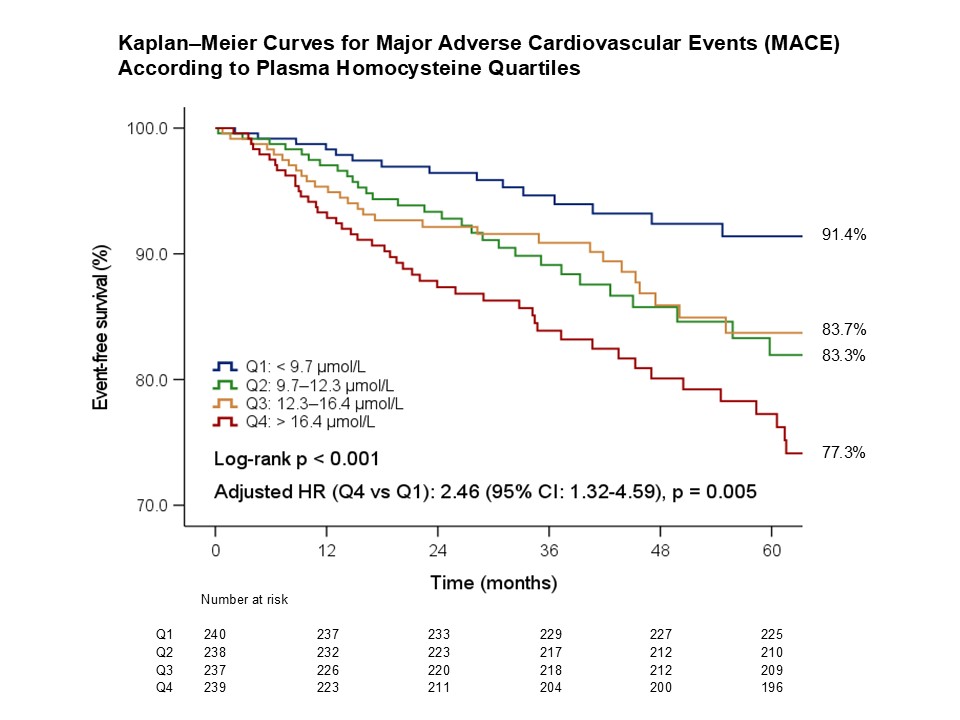
Conclusion
In the DES era, elevated plasma homocysteine independently predicts long-term adverse cardiovascular outcomes after PCI. Routine homocysteine assessment may enhance post-PCI risk stratification and guide personalized long-term management strategies in patients with coronary artery disease.