Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251024_0002
Comparison of Wire-Based Hyperemia-Induced Fractional Flow Reserve (FFR) and Angiography-Based Vessel Fractional Flow Reserve (vFFR) in Patients Who Underwent Physiological Assessment of Coronary Lesions
By Harilalith Kovvuri, Judah Nijas Arul, Akshay Prashanth Giri, Sadhanandham Shamugasundaram, Ramesh Sankaran, Nagendra Boopathy Senguttuvan
Presenter
Harilalith Kovvuri
Authors
Harilalith Kovvuri1, Judah Nijas Arul1, Akshay Prashanth Giri1, Sadhanandham Shamugasundaram1, Ramesh Sankaran1, Nagendra Boopathy Senguttuvan1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1
View Study Report
ABS20251024_0002
FFR
Comparison of Wire-Based Hyperemia-Induced Fractional Flow Reserve (FFR) and Angiography-Based Vessel Fractional Flow Reserve (vFFR) in Patients Who Underwent Physiological Assessment of Coronary Lesions
Harilalith Kovvuri1, Judah Nijas Arul1, Akshay Prashanth Giri1, Sadhanandham Shamugasundaram1, Ramesh Sankaran1, Nagendra Boopathy Senguttuvan1
Sri Ramachandra Institute of Higher Education and Research, India1
Background
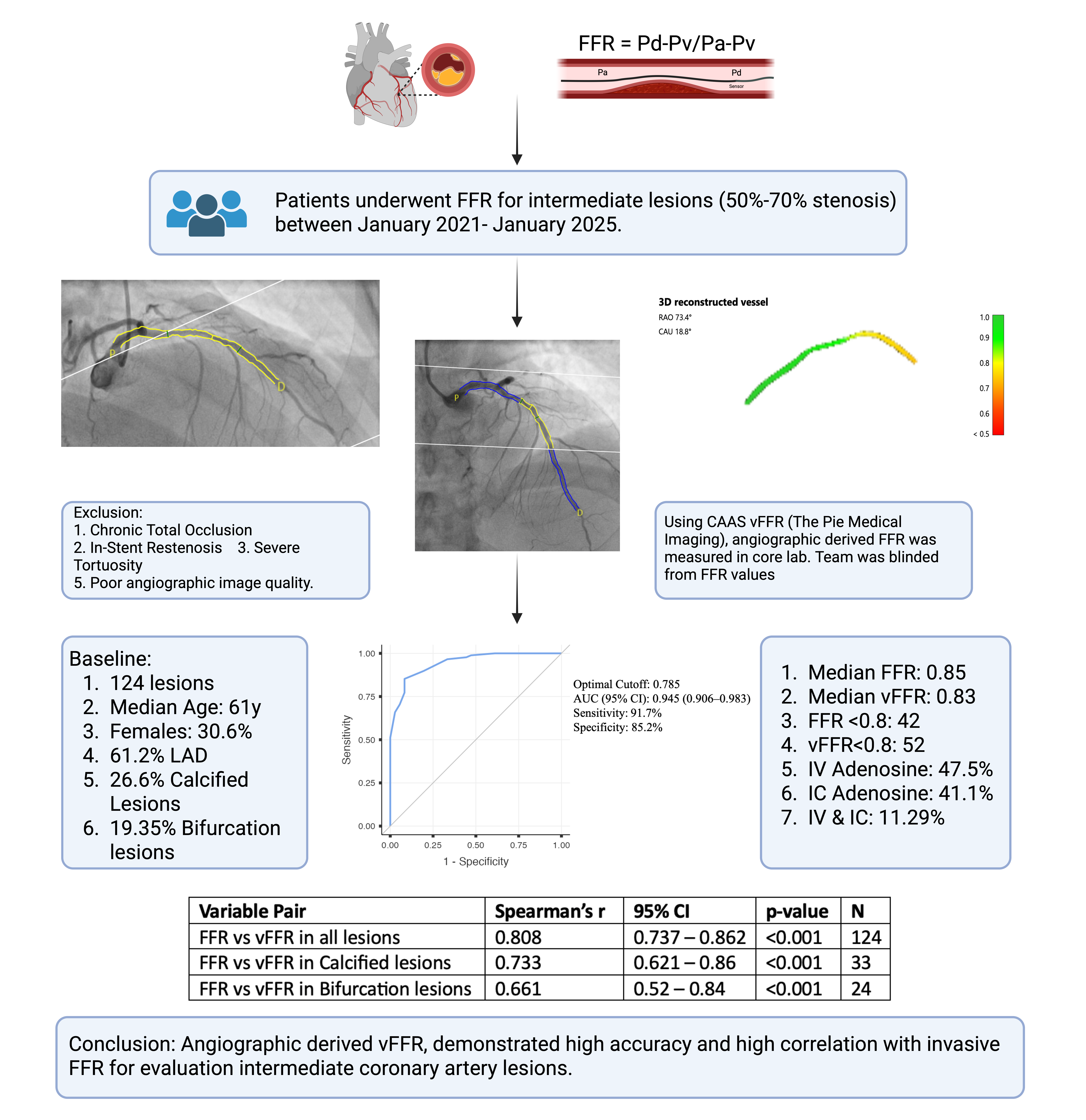
Despite robust evidence supporting physiology-guided revascularisation, the use of pressure wire-based fractional flow reserve (FFR) remains low due to procedural complexity, hyperemic requirements and patient discomfort. Angiography-derived vessel FFR (vFFR), using CAAS vFFR (Pie Medical Imaging, The Netherlands), a novel software developed based on three-dimensional quantitative coronary angiography (3D QCA), offers a wire-free, non hyperemic alternative. This study aimed to evaluate the diagnostic accuracy of vFFR against invasive FFR in assessing intermediate coronary lesions.
Methods
This study evaluated the concordance between angiography-derived vFFR and invasive FFR in patients with intermediate coronary stenosis. Retrospectively, coronary angiograms of patients who underwent adenosine based FFR from January 2022 until January 2025, for borderline lesions, were retrieved from the health management information system (HIMS) software and processed by a blinded core laboratory for vFFR computation. vFFR ≤0.80 denoted haemodynamic significance. The primary analysis was the correlation between vFFR and invasive FFR, assessed using Spearman’s correlation coefficient. Diagnostic performance of vFFR for detecting FFR-positive lesions was assessed using receiver operating characteristic (ROC) curve analysis, with calculation of area under the curve (AUC), sensitivity, specificity. Univariate analysis was done using Mann Whitney U test (for continuous variables) and Chi Square test (for categorical variables). Binary logistic regression analysis was done. All statistical analyses were performed using SPSS version 29 (IBM Corp., Armonk, NY, USA). A two-sided p-value <0.05 was considered statistically significant.
Results
Of 124 lesions (109 patient), Median Age is 61y and Females were 30.6%. Diabetes mellitus and systemic hypertension were present in 55.6% and 62.1% respectively. Most common presentation being Stable angina (40.3%), followed by NSTEMI (21%). Majority (61.2%) lesion were in LAD, the common vessel segment being Mid (37%), followed by proximal (35.4%). Calcified and bifurcation lesions were 26.6% and 19.35% respectively. Intravenous adenosine was used in 47.5%, Intracoronary in 41.1%, both in rest for invasive FFR. Median invasive FFR and vFFR were 0.85 (IQR 0.78 - 0.91) and 0.83 (IQR 0.76 - 0.91), respectively. vFFR demonstrated a strong correlation with invasive FFR (r = 0.81, p < 0.001) with excellent diagnostic accuracy (AUC 0.945), sensitivity 91.7%, specificity 85.2% and NPV 96.2%. Concordance was achieved in 82.3% of lesions. Correlation remained robust in non-calcified (r = 0.83, p < 0.001) and large vessels (r = 0.82, p < 0.001) but attenuated in calcified (r = 0.73, p < 0.001) and bifurcation lesions (r = 0.66, p < 0.001).
Conclusion
vFFR demonstrated excellent correlation with wire-based FFR, supporting its role as a practical, wire-free physiological tool for intermediate lesion assessment. Calcification remain key determinant of discordance. These findings reinforce the growing evidence for integrating angiography-derived physiology into routine PCI planning.