Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20251002_0001
Ambidextrous Guide Catheter Strategy in Primary Percutaneous Coronary Intervention for St-Elevation Myocardial Infarction: Effects on Reperfusion Time, Procedural Efficiency, and Safety
By Florimond Joseph Martin Garcia Jr.
Presenter
Florimond Joseph Martin Garcia Jr.
Authors
Florimond Joseph Martin Garcia Jr.1
Affiliation
The Medical City, Philippines1
View Study Report
ABS20251002_0001
ACS/AMI
Ambidextrous Guide Catheter Strategy in Primary Percutaneous Coronary Intervention for St-Elevation Myocardial Infarction: Effects on Reperfusion Time, Procedural Efficiency, and Safety
Florimond Joseph Martin Garcia Jr.1
The Medical City, Philippines1
Background
ST-elevation myocardial infarction (STEMI) is a time-sensitive emergency where the rapid restoration of coronary blood flow through primary percutaneous coronary intervention (PCI) is critical to improving patient outcomes. Delays in reperfusion are directly associated with increased infarct size, worse ventricular function, and higher mortality. Despite significant advances in interventional cardiology, real-world practice often faces challenges in consistently meeting recommended reperfusion targets.In routine clinical settings, many operators employ a conventional diagnostic-to-guide catheter approach, beginning angiography with a diagnostic catheter before exchanging to a guide catheter for intervention. While widely practiced, this two-step workflow inevitably introduces an additional exchange, which may prolong reperfusion time and add to overall procedure duration. In the acute STEMI scenario, where every minute of ischemia translates to potential myocardial damage, this inefficiency could negatively affect clinical outcomes.The ambidextrous guide catheter offers a potential solution by functioning as both a diagnostic and interventional catheter. This strategy allows operators to perform diagnostic angiography and immediately proceed with intervention without the need for catheter exchange. By simplifying the workflow, the use of an ambidextrous guide catheter may reduce reperfusion delays, shorten total procedural duration, and still maintain high technical success with acceptable safety profiles.Clinical data directly comparing ambidextrous guide catheters with the conventional diagnostic-to-guide approach in the primary PCI setting remain limited. To address this gap, we conducted a retrospective analysis of consecutive STEMI cases at our institution, comparing procedural efficiency, complications, and in-hospital outcomes between these two strategies.
Methods
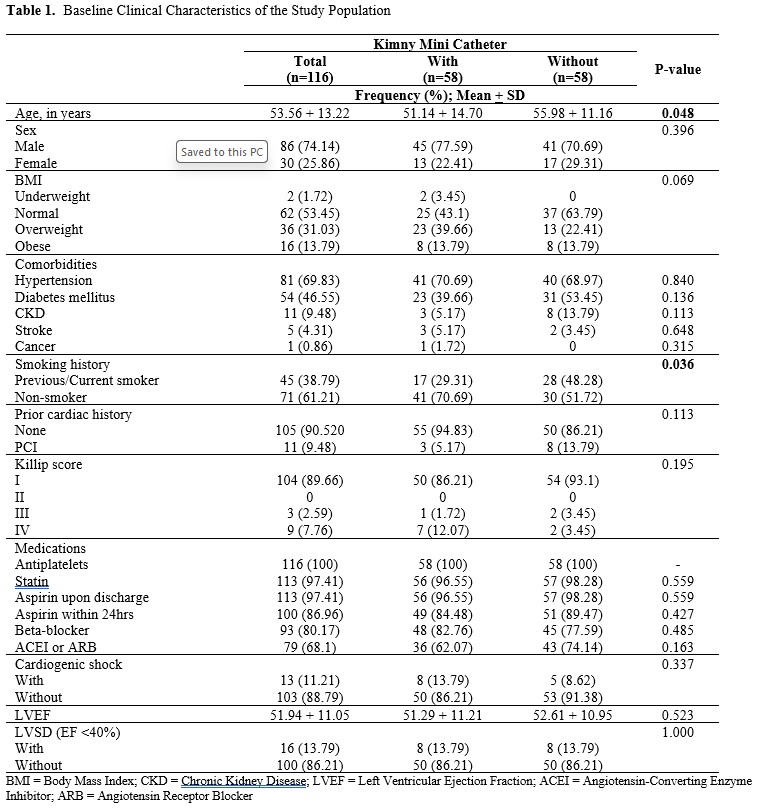
This was a retrospective, real-world study of consecutive patients with ST-elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) at The Medical City, a tertiary referral center, between January 2022 and June 2024. All STEMI cases treated with primary PCI during this period were included without exclusions, reflecting routine practice and enabling a true all-comer analysis. Patients were categorized according to the initial catheterization strategy: those treated from the outset with an ambidextrous guide catheter (n = 58) and those treated with the conventional diagnostic-to-guide exchange approach (n = 58).
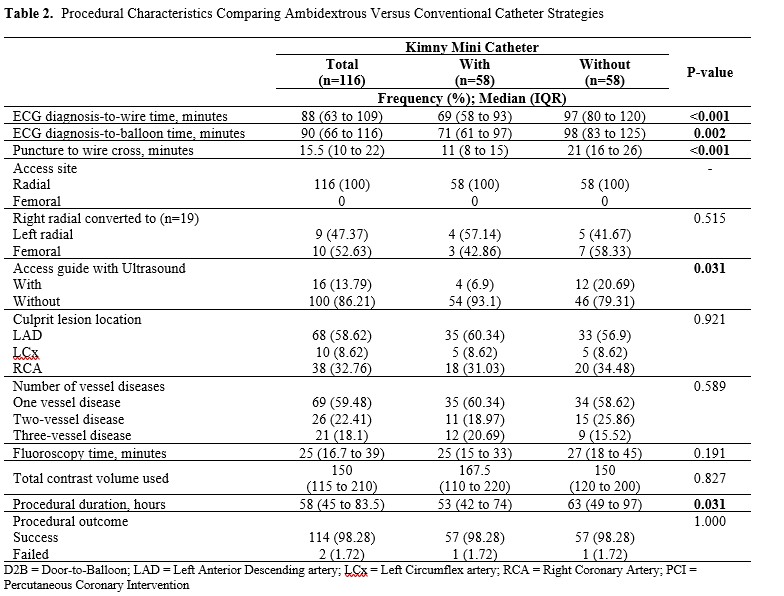
We systematically collected demographic data, cardiovascular risk factors, clinical presentation, angiographic findings, and procedural characteristics from electronic medical records and the institutional STEMI registry. Key procedural efficiency metrics included puncture-to-wire cross, diagnosis-to-wire, diagnosis-to-balloon, and total procedure duration. Fluoroscopy time and contrast volume were also recorded to provide additional measures of efficiency.
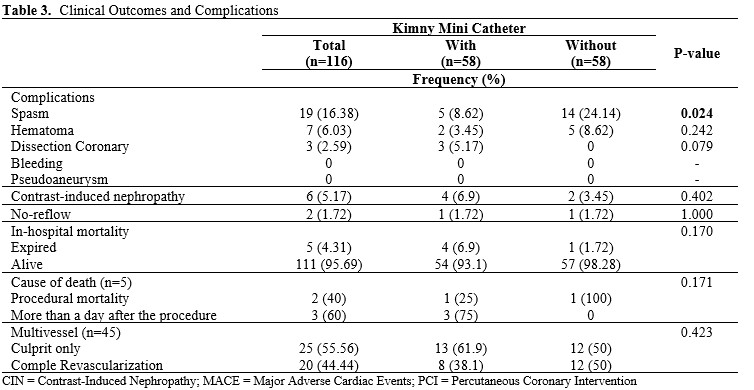
Safety outcomes comprised vascular access complications, coronary complications such as dissection, perforation, or no-reflow, and in-hospital adverse events including reinfarction, stroke, or death. Data were independently reviewed and validated to ensure accuracy.
Comparisons between groups were performed using chi-square or Fisher’s exact test for categorical variables and Student’s t-test for continuous variables, with two-tailed p < 0.05 considered statistically significant. All analyses were conducted using SPSS version 27 (IBM Corp, Armonk, NY, USA). This study design provided a direct and unbiased comparison of efficiency and safety between the ambidextrous and conventional catheter strategies in a consecutive STEMI population.
Results
Baseline demographic, clinical, and angiographic characteristics were well balanced between groups, with no significant differences in age, sex, cardiovascular risk factors, or culprit lesion distribution, ensuring that observed outcomes reflected catheter strategy rather than baseline imbalances.The ambidextrous approach significantly reduced key procedural time intervals. Puncture-to-wire cross was shorter compared with the conventional diagnostic-to-guide strategy (11 vs 21 minutes, p < 0.001). Diagnosis-to-wire and diagnosis-to-balloon times were also reduced by approximately 28 and 27 minutes, respectively. Total procedural duration was shorter in the ambidextrous group (53 vs 63 minutes, p = 0.03). Fluoroscopy time and contrast volume were similar, confirming that the observed efficiency gains were related to workflow rather than case complexity. The consistent reduction in reperfusion-related intervals underscores the potential for this strategy to facilitate faster reperfusion in routine practice.Procedural success exceeded 95% in both groups. Complications were less frequent with the ambidextrous catheter (8.6% vs 24.1%, p = 0.02), driven mainly by fewer vascular access and catheter-related events. Coronary complications such as dissection and no-reflow were rare and showed no significant differences, suggesting that procedural streamlining did not increase coronary risk.In-hospital mortality was low overall. Although numerically higher in the ambidextrous group (6.9% vs 1.7%), this difference was not statistically significant (p = 0.17). Reinfarction and stroke were rare events and occurred at similar rates between the two groups.
Conclusion
Overall, use of an ambidextrous guide catheter in primary percutaneous coronary intervention for ST-elevation myocardial infarction was associated with faster reperfusion workflow and fewer complications, while maintaining high procedural success and comparable in-hospital outcomes. This simplified single-catheter approach may help optimize efficiency in real-world STEMI care and warrants validation in larger, prospective multicenter studies.