Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20250927_0001
Clinical Outcomes of Atherectomy PCI With Hybrid Dcb Therapy: A Single-Center Retrospective Study
By Noor Yuhyi Sulaiman, Tawfeq Mohd Noor, Zulaikha Zainai, Ganapathi Palaniappan, Hafidz Hadi
Presenter
Noor Yuhyi Sulaiman
Authors
Noor Yuhyi Sulaiman1, Tawfeq Mohd Noor1, Zulaikha Zainai1, Ganapathi Palaniappan1, Hafidz Hadi1
Affiliation
Institut Jantung Negara, Malaysia1
View Study Report
ABS20250927_0001
Calcified Lesion
Clinical Outcomes of Atherectomy PCI With Hybrid Dcb Therapy: A Single-Center Retrospective Study
Noor Yuhyi Sulaiman1, Tawfeq Mohd Noor1, Zulaikha Zainai1, Ganapathi Palaniappan1, Hafidz Hadi1
Institut Jantung Negara, Malaysia1
Background
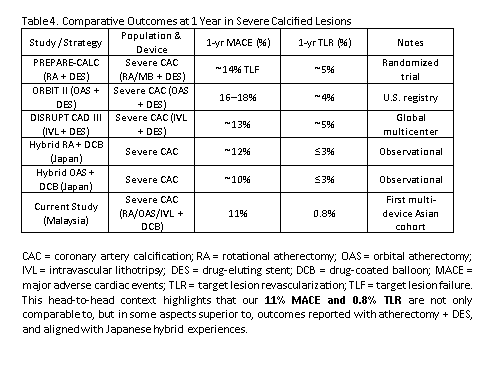
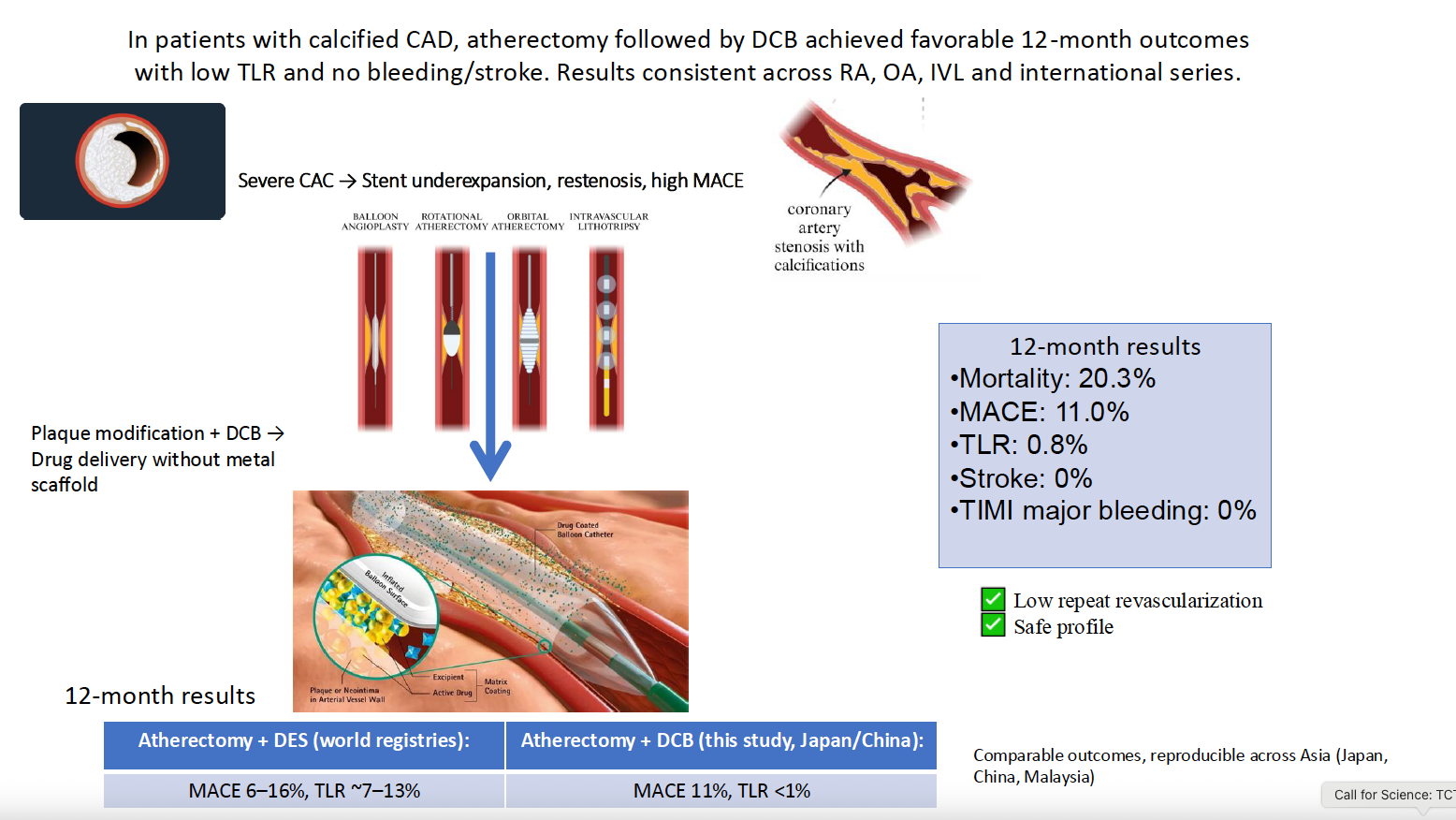
Severe coronary artery calcification (CAC) remains one of the most challenging substrates for PCI, leading to impaired device delivery, suboptimal stent expansion, and worse clinical outcomes. In contemporary practice, atherectomy plus stenting with new-generation drug-eluting stents (DES) is the dominant strategy. Yet even with plaque modification, outcomes remain inferior to those in non-calcified lesions.
Methods
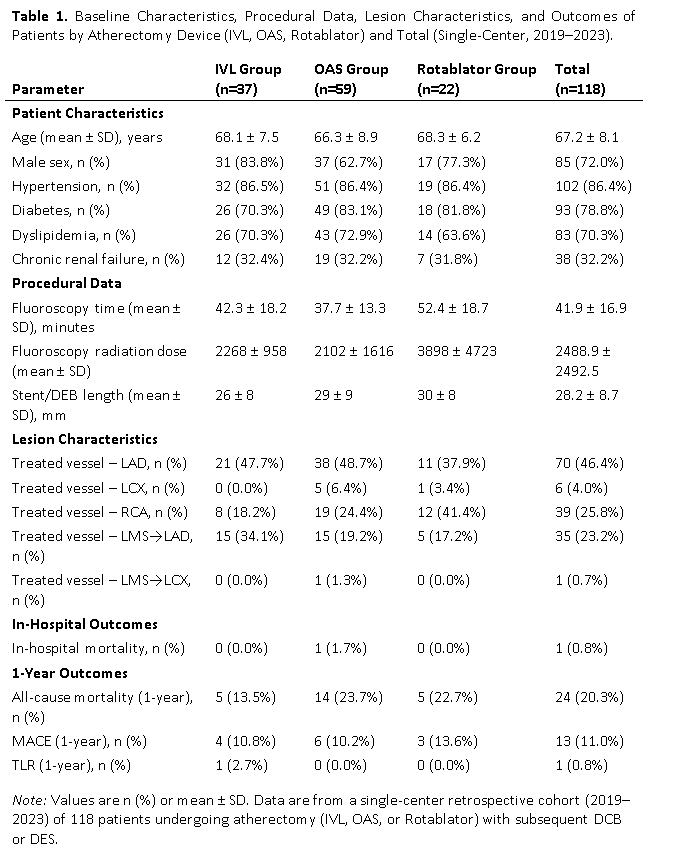
Study Design and PopulationWe retrospectively analyzed patients with severe coronary artery calcification undergoing PCI at Institut Jantung Negara from January 2021 to December 2023. Inclusion criteria: angiographically severe calcification requiring lesion modification with atherectomy. Patients were divided into two groups: atherectomy followed by drug-coated balloon (DCB) angioplasty and atherectomy followed by drug-eluting stent (DES) implantation. Atherectomy device selection (rotational, orbital, or intravascular lithotripsy) was at operator discretion. Procedural success was defined as <30% residual stenosis without in-hospital major adverse cardiac events (MACE). The primary endpoint was MACE at 12 months (composite of cardiac death, myocardial infarction, and target lesion revascularization). Secondary endpoints included target lesion failure (TLF), target lesion revascularization (TLR), and procedural outcomes. Clinical follow-up was performed at 1, 6, and 12 months. Kaplan–Meier analysis was used to estimate event-free survival; between-group differences were evaluated with log-rank testing. Baseline demographics, angiographic characteristics, and outcomes were compared using chi-square or Fisher’s exact test for categorical variables and Student’s t test or Mann–Whitney U test for continuous variables, as appropriate. A p value <0.05 was considered statistically significant.
Results
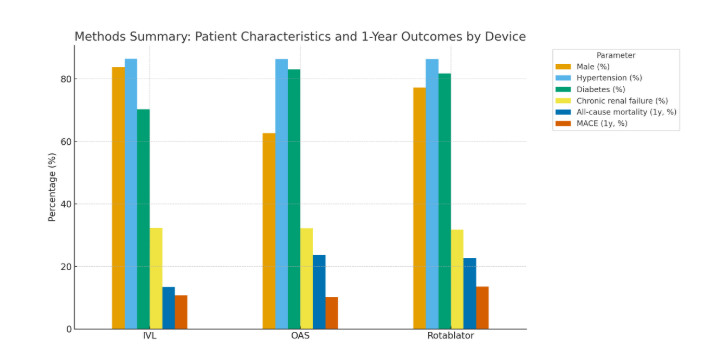
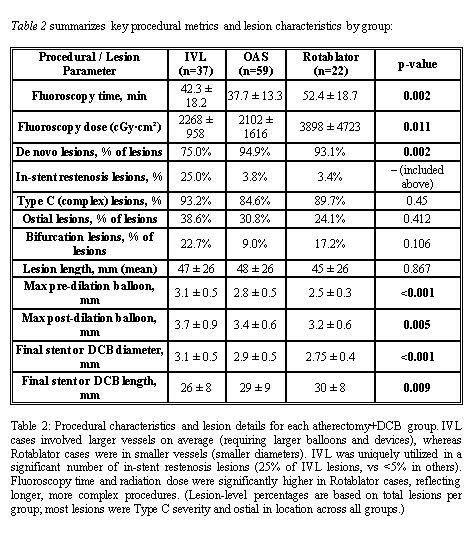
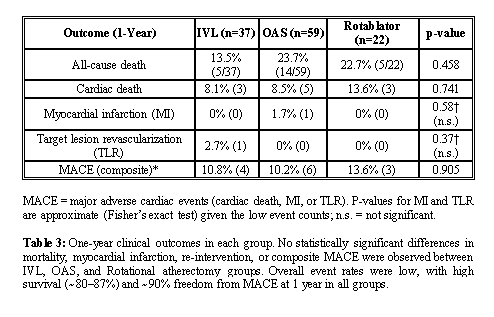
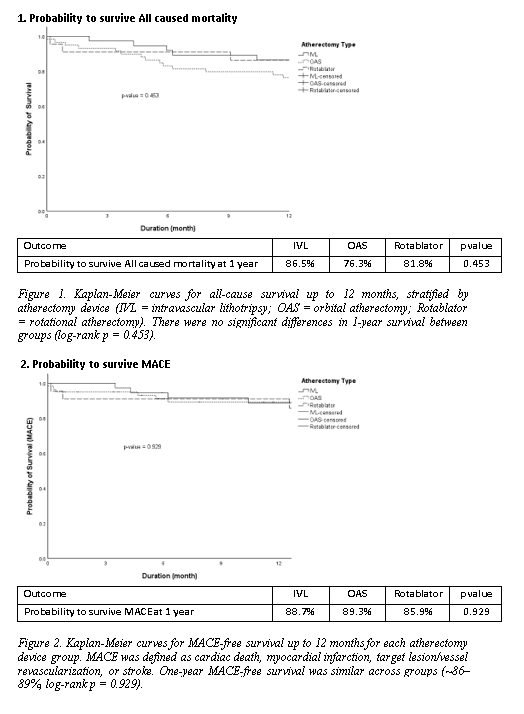
A total of 118 patients were included: IVL (n=37), OAS (n=59), and Rotablator (n=22). Mean age was 67 ± 8 years, and 72% were male. Cardiovascular risk factors were common: hypertension (86%), diabetes (79%), dyslipidemia (70%), and chronic renal failure (32%).Lesion distribution involved LAD in 46%, RCA in 26%, and LMS–LAD in 23%. Most lesions were de novo (89%) and type C (88%), with bifurcation in 15% and CTO in 4%. Mean lesion length was 47 ± 26 mm.Procedural success was achieved in 98%. Fluoroscopy time was shortest with OAS (37.7 ± 13.3 min) and longest with Rotablator (52.4 ± 18.7 min, p = 0.002). Radiation dose was significantly higher with Rotablator (3898 ± 4723 vs. 2102 ± 1616 with OAS and 2268 ± 958 with IVL, p = 0.011).In-hospital mortality was 0.8% (1 patient, OAS group). At 1 year, all-cause mortality was 20.3% (13.5% IVL, 23.7% OAS, 22.7% Rotablator; p = 0.458). MACE occurred in 11.0% overall, with no significant difference between groups (10.8% IVL, 10.2% OAS, 13.6% Rotablator; p = 0.905). TLR was rare (0.8%, one patient in IVL group). Kaplan–Meier analysis showed similar survival for both all-cause mortality (86.5% IVL vs. 76.3% OAS vs. 81.8% Rotablator; p = 0.453) and MACE-free survival (88.7% IVL vs. 89.3% OAS vs. 85.9% Rotablator; p = 0.929).Overall, outcomes of atherectomy + DCB strategy were consistent across devices, with comparable 1-year mortality and MACE rates to international reports.
Conclusion
In a real-world Asian cohort with severe coronary calcification, atherectomy-facilitated DCB PCI yielded low ischemic complications, very low repeat revascularization (TLR 0.8%), and acceptable survival despite high comorbidity burden. Importantly, outcomes were consistent across IVL, OAS, and RA, supporting the principle that adequate lesion preparation—rather than device choice—drives success when pursuing a stent-sparing strategy.