Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
ABS20250723_0001
Association of LMWH Bridging With Clinical Outcomes in Patients With Venous Thromboembolism Treated With Direct Oral Anticoagulants: A Nationwide Cohort Study
By Jung-Chi Hsu, Jen-Kuang Lee
Presenter
Jung-Chi Hsu
Authors
Jung-Chi Hsu1, Jen-Kuang Lee2
Affiliation
National Taiwan University Hospital Jinshan Branch, Taiwan1, National Taiwan University Hospital, Taiwan2
View Study Report
ABS20250723_0001
Pharmacotherapy (Innovation)
Association of LMWH Bridging With Clinical Outcomes in Patients With Venous Thromboembolism Treated With Direct Oral Anticoagulants: A Nationwide Cohort Study
Jung-Chi Hsu1, Jen-Kuang Lee2
National Taiwan University Hospital Jinshan Branch, Taiwan1, National Taiwan University Hospital, Taiwan2
Background
The role of low-molecular-weightheparin (LMWH) bridging during direct oral anticoagulant (DOAC) initiation forvenous thromboembolism (VTE) remains unclear. We evaluated whether bridgingaffects short-term outcomes in hospitalized VTE patients.
Methods
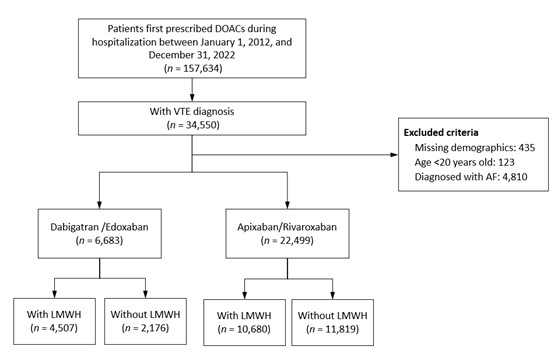
We conducted a retrospective cohortstudy using Taiwan’s national hospitalization database from 2012 to 2022.Adults hospitalized for VTE and newly prescribed DOAC were included. Propensityscore matching was performed by DOAC type based on LMWH bridging.
Results
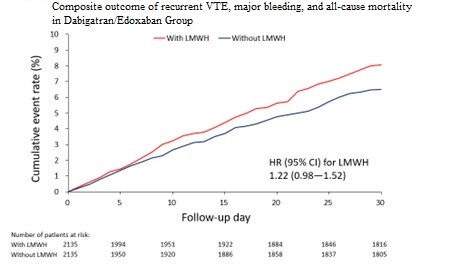
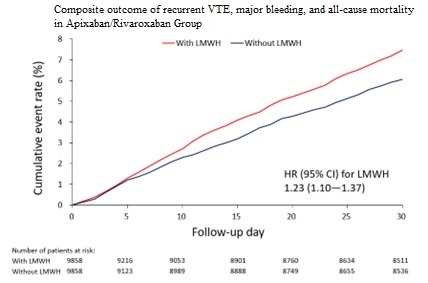
Among 29,182 patients, 6,683received dabigatran/edoxaban and 22,499 apixaban/rivaroxaban. Bridging was morefrequent in patients with active cancer or concurrent pulmonary embolism anddeep vein thrombosis. In the dabigatran/edoxaban group, bridging was notassociated with differences in recurrent VTE, cardiovascular mortality, orall-cause mortality (SHR 1.41 [0.90–2.21], p = 0.136; 0.67 [0.44–1.01], p =0.058; 1.16 [0.89–1.53], p = 0.275). In the apixaban/rivaroxaban group,bridging was associated with a higher risk of acute myocardial infarction (SHR3.37 [1.24–9.13], p = 0.017) and recurrent VTE (SHR 1.81 [1.48–2.23], p <0.001), mainly driven by recurrent deep vein thrombosis (SHR 2.07 [1.63–2.64],p < 0.001). Cardiovascular mortality was lower in the bridged group (SHR0.73 [0.59–0.89], p = 0.002), while all-cause mortality was similar (SHR 1.04[0.91–1.19], p = 0.597).
Conclusion
LMWH bridging was not associated with short-termoutcome differences in dabigatran/edoxaban users. In contrast, bridging inapixaban/rivaroxaban users was linked to higher thrombotic risk, particularly recurrent deep vein thrombosis, despite lower cardiovascular mortality.Bridging decisions should consider DOAC type and patient profile.