
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-028
Bifurcation Stenting Technique With Angulated Side Branch in Presence of in Stent Re-Stenosis With Drug Eluting Stent & Drug Coated Balloon
By Hariom Tyagi
Presenter
Hariom Tyagi
Authors
Hariom Tyagi1
Affiliation
Lokpriya Hospital, India1,
View Study Report
TCTAP C-028
Coronary - Complex PCI - Bifurcation
Bifurcation Stenting Technique With Angulated Side Branch in Presence of in Stent Re-Stenosis With Drug Eluting Stent & Drug Coated Balloon
Hariom Tyagi1
Lokpriya Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
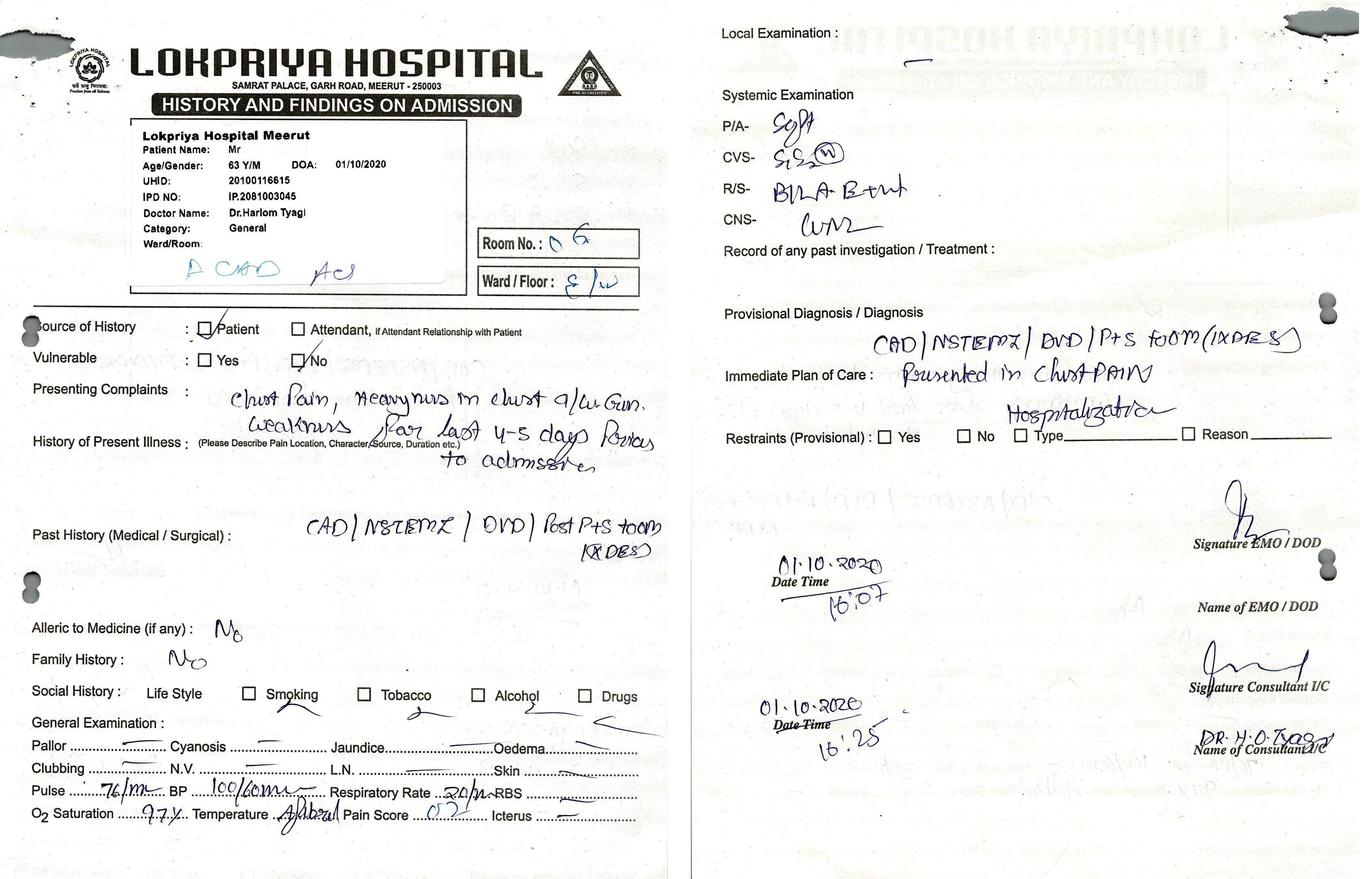
A 63 years old male patient presented herewith C/O Chest pain, heaviness in Chest, associated with generalized weakness for last 4-5 days, symptoms increased 2 hours prior to admission. H/O- CAD/ACS/NSTEMI (RECENT)/USA/POST CAG- DVD/POST PTCA TO OM (19.05.2020).
Relevant Test Results Prior to Catheterization
ECG shows Non specific changes. 2D-ECHO suggestive of No RWMA. Adequate LV Systolic Function (LVEF=55%). In view of Symptoms & Diagnosis, plan for CAG.
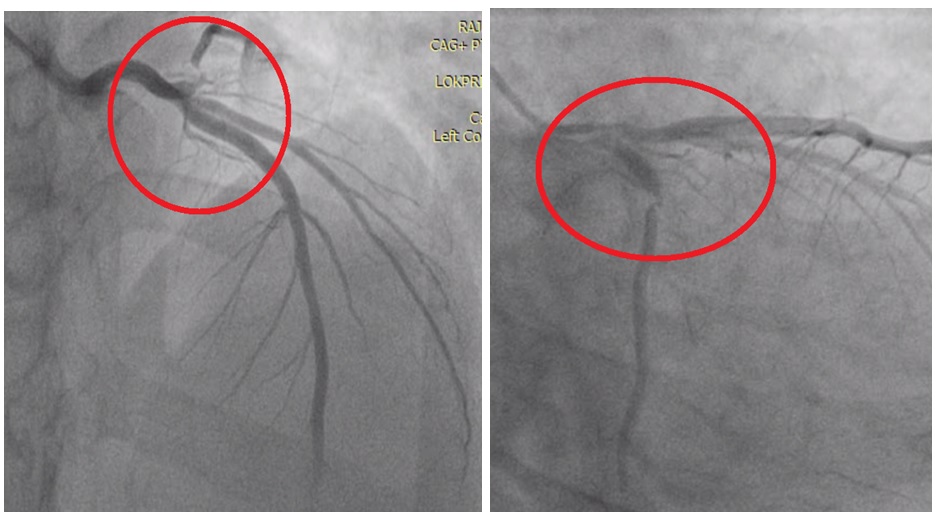
Relevant Catheterization Findings
Double Vessel Disease with 100% ISR in OM2: Left Main: Normal. LAD: Type III vessel, Proximal 50% disease. D1: Ostioproximal 50% disease. D2: Normal. LCX: Co-dominant, Distal 99% disease at OM Bifurcation. OM1: Small size normal. OM2: 100% ISR in Ostioproximal. RCA: Co-dominant, Normal. PLV/PDA: Normal. Plan for PTCA to LCX & OM Bifurcation.
Interventional Management
Procedural Step
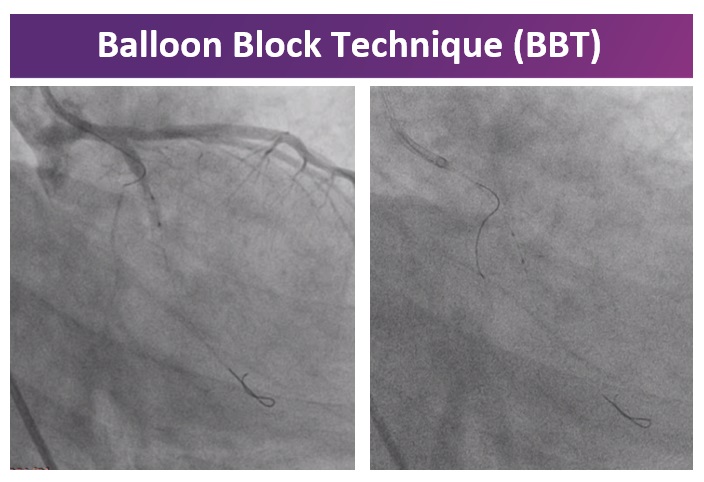
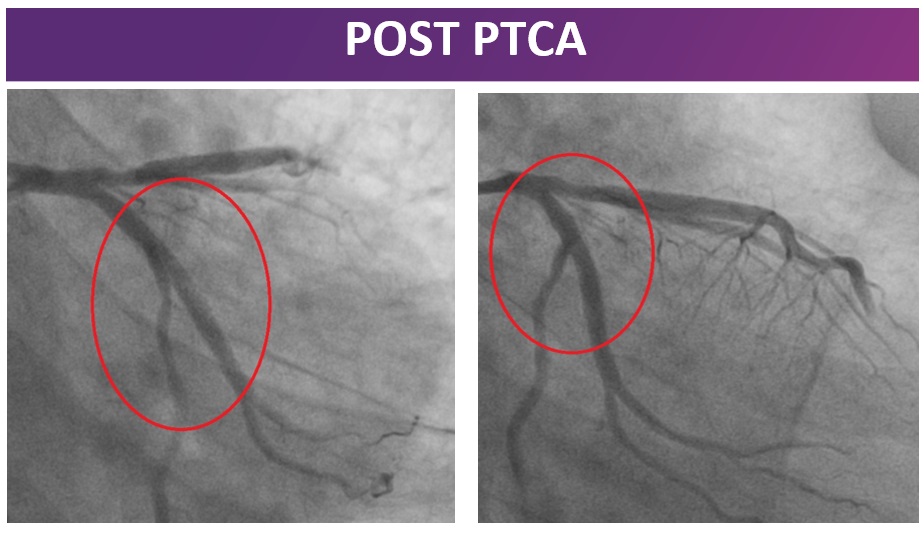
Left Coronary Artery was engaged with EBU 3.5, 6F guide catheter. A 0.014” SION BLUE wire was used to cross the OM lesion. Pre dilation done with SC Sapphire Balloon 2.0 × 10 mm & 2.75 × 10 mm @ 12 atmosphere. A 0.014” PILOT 50 wire used to cross in LCX. Pre dilation done with SC Sapphire Balloon 1.5 × 10 mm @ 12 atmosphere & 2.0 × 10 mm @ 12 atmosphere at bifurcation than a SC Sapphire Balloon 2.0 × 10 mm cross in LCX lesion and simultaneous NC Sapphire Balloon 2.75 × 10 mm cross in OM lesion and kissing dilatation done in OM & LCX lesion. After that a Drug Eluting Stent RESOLUTE ONYX 3.0 × 34 mm deployed in LCX to OM @ 12 atmosphere. After that 0.014” SION BLUE wire exchange in LCX and a 0.014” SION BLUE wire cross in OM. Post dilation done of OM stent with NC Sapphire Balloon 3.5 × 10 mm @ 12 atmosphere. Then dilatation done with SC Sapphire Balloon 1.5 × 10 mm & 2.0 × 10 mm @ 12 atmosphere in LCX at bifurcation LCX & OM. After that a Drug Eluting balloon MOZEC SEB 2.75 × 17 mm dilated in LCX at bifurcation @ 10 atmosphere. GP IIb IIIa inhibitor was used during the procedure. Excellent result with TIMI III flow achieved. Successful PTCA with stenting to LCX to OM and DEB to LCX side branch.
Case Summary
Restenosis post bifurcation PCI remain one of the most challenging lesions particularly for the side branches in terms of long term procedural success rate. Drug eluting balloon provide novel therapeutic strategy for bifurcation restenosis for side branch Ostium. In-stent restenosis is the most important limitation of modern coronary angioplasty. Drug-eluting stents solve this problem but at the cost of late stent thrombosis and longer duration of dual-antiplatelet therapy. Drug-Eluting Balloon (DEB) technology is now available and offers an attractive option for treatment of restenosis.