
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-158
A Challenging Case Report: Coronary Intervention in a Female With Aortic Aneurysm
By Chia-Ling Tsai
Presenter
chia-ling tsai
Authors
Chia-Ling Tsai1
Affiliation
MacKay Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-158
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
A Challenging Case Report: Coronary Intervention in a Female With Aortic Aneurysm
Chia-Ling Tsai1
MacKay Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
56-year-old female with past history of AsAo grafting and emergent CABG was performed from the graft to distal RCA using SVG.
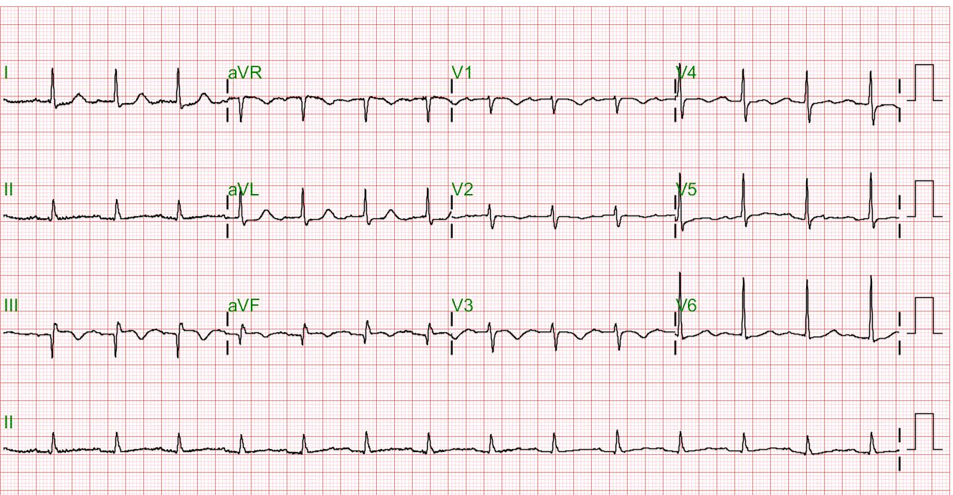
Chief complaints: sudden onset chest tightness. The relation symptoms were dyspnea, palpitation, cold sweating.
One week later after discharged under the diagnosis of 1. NSTEMI 2.CAD with SVD stauts post successful PCI, re-admission due to acute chest pain and dizziness

Relevant Test Results Prior to Catheterization
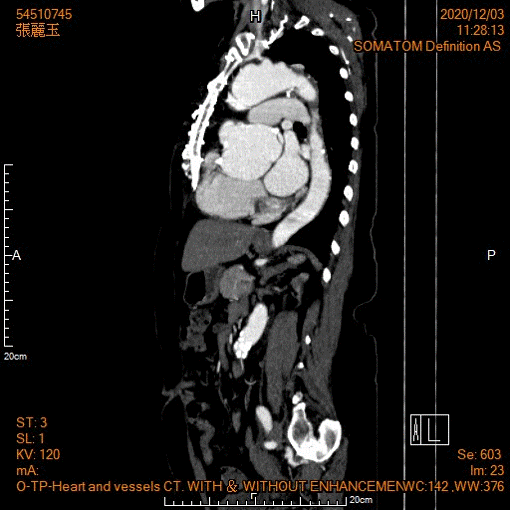
Aortic root aneurysm s/p stenting at ascending aorta
Echocardiography : new regional wall motion abnormality at anterior wall
Echocardiography : new regional wall motion abnormality at anterior wall
Relevant Catheterization Findings
1.Patent right coronary artery 2.
Aortic dissection flap compress ostium left main


Interventional Management
Procedural Step
Coronary angiography : Patent left coronary artery but can not engage well under JL-5 catheter due to aortic aneurysm os-RCA 90% stenosis, TIMI II flow
SVG graft to distal RCA total occlusion
Intervention: IVUS guide, DES 4.5 x 18 mm at ostium RCA
Intervention:Due to dilated aortic root, we use JL 5.0 guiding catheter for engaging to LM orificeThen we manipulate Runthrough EF wire to distal LAD.


Intervention: IVUS guide, DES 4.5 x 18 mm at ostium RCA
One week later,
Coronary angiography :
Patent right coronary artery
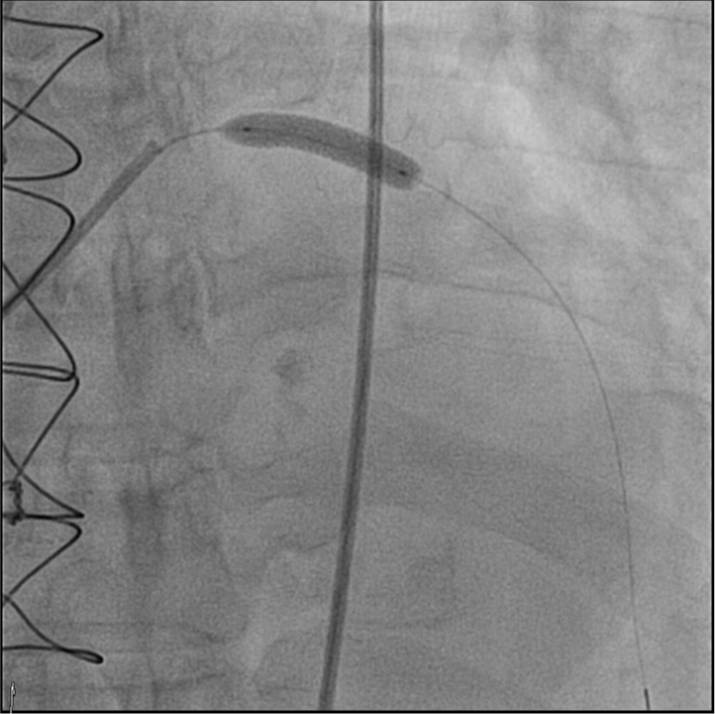
Aortic dissection flap compress ostium left main Intervention:Due to dilated aortic root, we use JL 5.0 guiding catheter for engaging to LM orificeThen we manipulate Runthrough EF wire to distal LAD.
Stenting: Onyx(DES) 5.0mm*22mm was inflated up to 8 atm at Left main
Then we used the stent balloon inflated at proximal stent up to 12 atm
Case Summary
A case of NSTEMI and CAD with SVD (os-RCS 90% stenosis) s/p PCI with DES in RCA.One week later, acute chest pain and dizziness developed for one day and admission again due to NSTEMI recurred.This time, aortic dissection flap compress ostium left main was noted and underwent successful percutaneous coronary intervention.