
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-196
Sleep Disturbing Painful Leg in Patient Who Underwent Bilateral IFP Artery Interventions 5 Times After Fem-Fem Bypass Surgery
By Wonmook Hwang, Jae-Hwan Lee
Presenter
Wonmook Hwang
Authors
Wonmook Hwang1, Jae-Hwan Lee1
Affiliation
Chungnam National University Sejong Hospital, Korea (Republic of)1,
View Study Report
TCTAP C-196
Endovascular - Other Endovascular Intervention
Sleep Disturbing Painful Leg in Patient Who Underwent Bilateral IFP Artery Interventions 5 Times After Fem-Fem Bypass Surgery
Wonmook Hwang1, Jae-Hwan Lee1
Chungnam National University Sejong Hospital, Korea (Republic of)1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
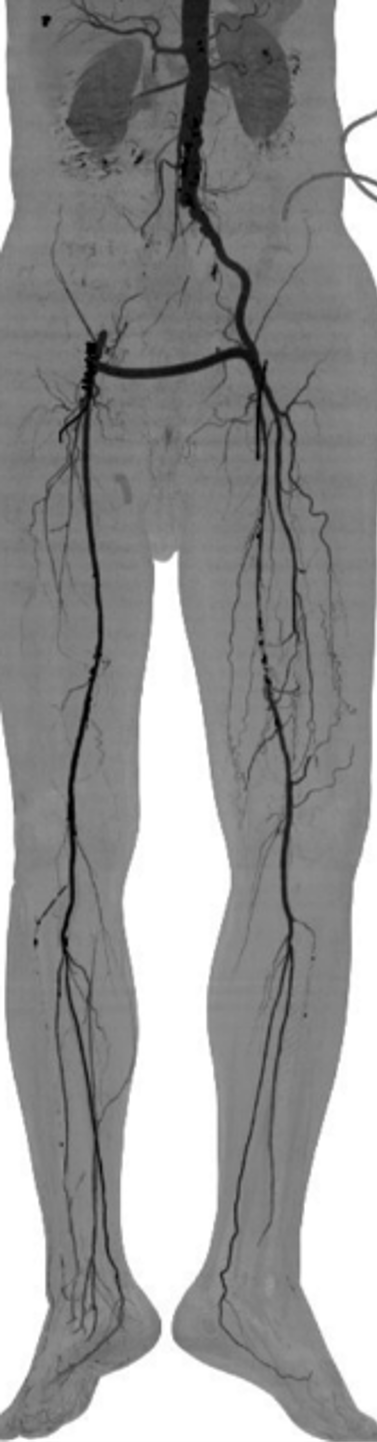
68 YO man whose risk factors for ASCVD are Current smoker, Dyslipidemia, Prediabetes came to outpatient clinic. He had resting leg pain in right side disturbing his sleeping and also had claudication on left leg within 20 meters of walking. According to the medical records from another hospital, he underwent a femoral to femoral bypass surgery because of right iliac CTP, left SFA stenosis in 2018.
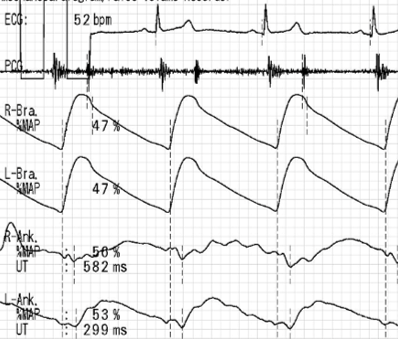
Relevant Test Results Prior to Catheterization
1.5 years later, he experienced severe both leg resting pain due to thrombotic occlusion in the right SFA. He underwent balloon angioplasty in the SFA, PA and PTA. 2 months later, resting pain of right leg recurred due to reocclusion, stenting on right iliac CTO leson and proximal SFA and POBA on m-dSFA and PA was done. 2 months later, in-stents reocclusion reoccured, so he had thrombectomy and atherectomy plus thrombolytics infusion. But 3 months later, both side stents and SFAs reoccluded.

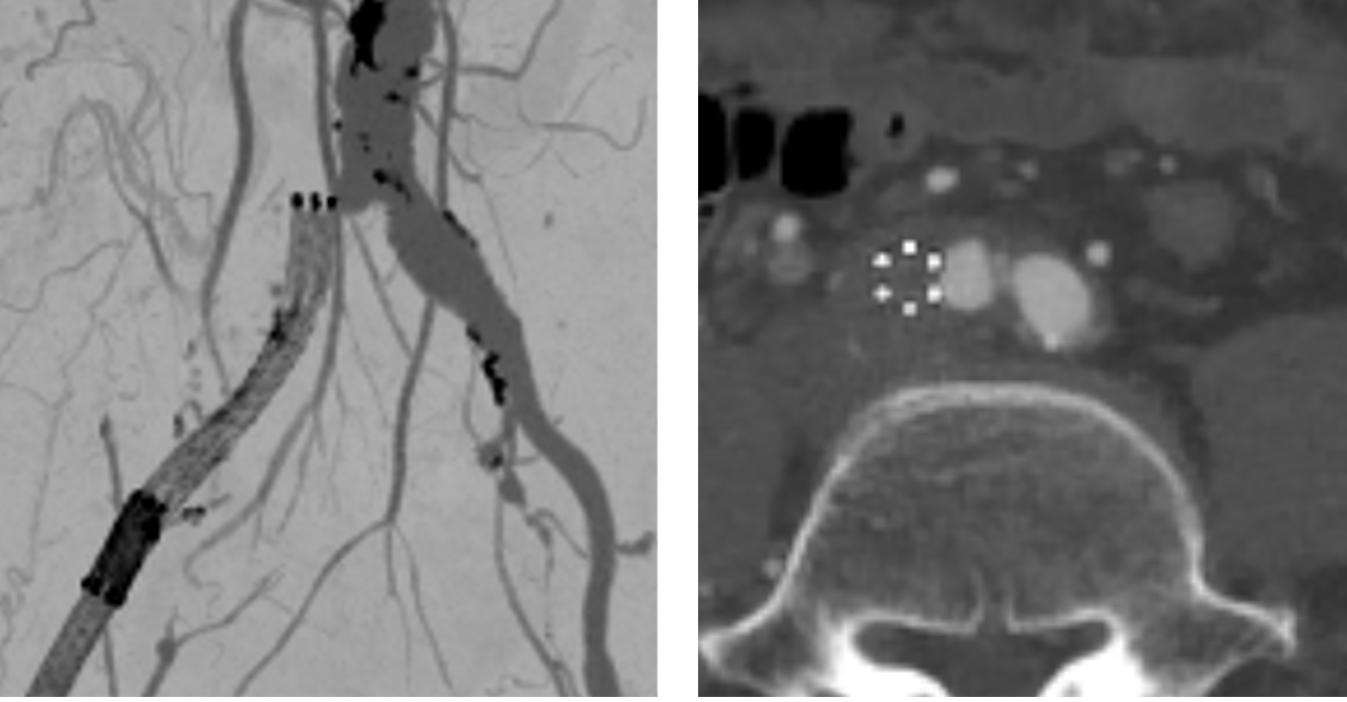
Relevant Catheterization Findings
Reviewed CT showed the right CIA ostial stent was subintimally located. With reviewd previous interventions(from other hospital), we found subintimal penetration of wire and distortion of iliac stent.

Interventional Management
Procedural Step
We decided to access thelesion via 2 access routes initially(radial + retrograde peroneal). Since CTOlesion was very long and old over 2 years, many sheaths and guidewires wereused to the ISR during lesion penetration. We used 150cm 5Fr MP, CXI microcatheter plus 0.014 Command ES, Stiff Terumo, Halberd 12g, Astato 40g. After wiring with balloon dilatation and balloon assisted Ansel sheath delivery, we did rotational atherectomyand thrombectomy before and after filter protection at P3 level. Four DCBs wereused on popliteal to iliac lesion, and balloon expandable stent was used on CIA ostium.



Case Summary
We did successfulrecanalization of chronic total right iliac in-stent reocclusion by balloon angioplasty with proximal spotstenting. And successfully recanalized right femoral-popliteal long chronic total occlusion with Jetstreamatherectomy and drug-coated balloon angioplasty.