
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-198
Utilizing Self-Radiopaque Technique and Greater Aortic Curvature Guidance for On-Table Fenestration in Zone 0 Thoracic Endovascular Aortic Repair for Aortic Arch Aneurysm: A Case Report With Vietnam National Heart Institute Approach
By Than Xuan Le, Tuan Minh Pham, Hung Manh Pham, Quang Ngoc Nguyen
Presenter
Than Xuan Le
Authors
Than Xuan Le1, Tuan Minh Pham1, Hung Manh Pham1, Quang Ngoc Nguyen1
Affiliation
Vietnam National Heart Institute, Vietnam1,
View Study Report
TCTAP C-198
Endovascular - Thoracic & Abdominal Aortic Interventions
Utilizing Self-Radiopaque Technique and Greater Aortic Curvature Guidance for On-Table Fenestration in Zone 0 Thoracic Endovascular Aortic Repair for Aortic Arch Aneurysm: A Case Report With Vietnam National Heart Institute Approach
Than Xuan Le1, Tuan Minh Pham1, Hung Manh Pham1, Quang Ngoc Nguyen1
Vietnam National Heart Institute, Vietnam1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
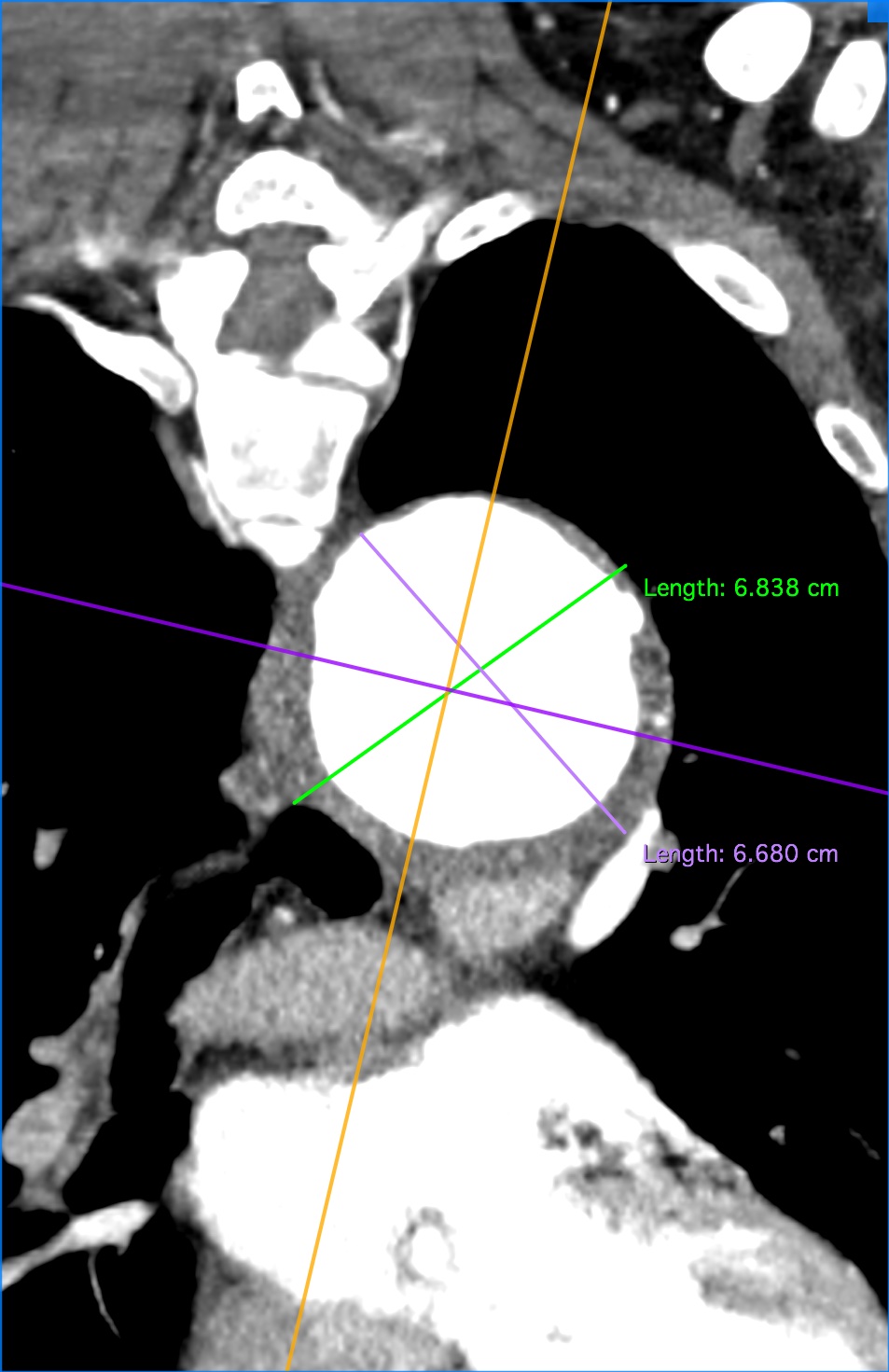
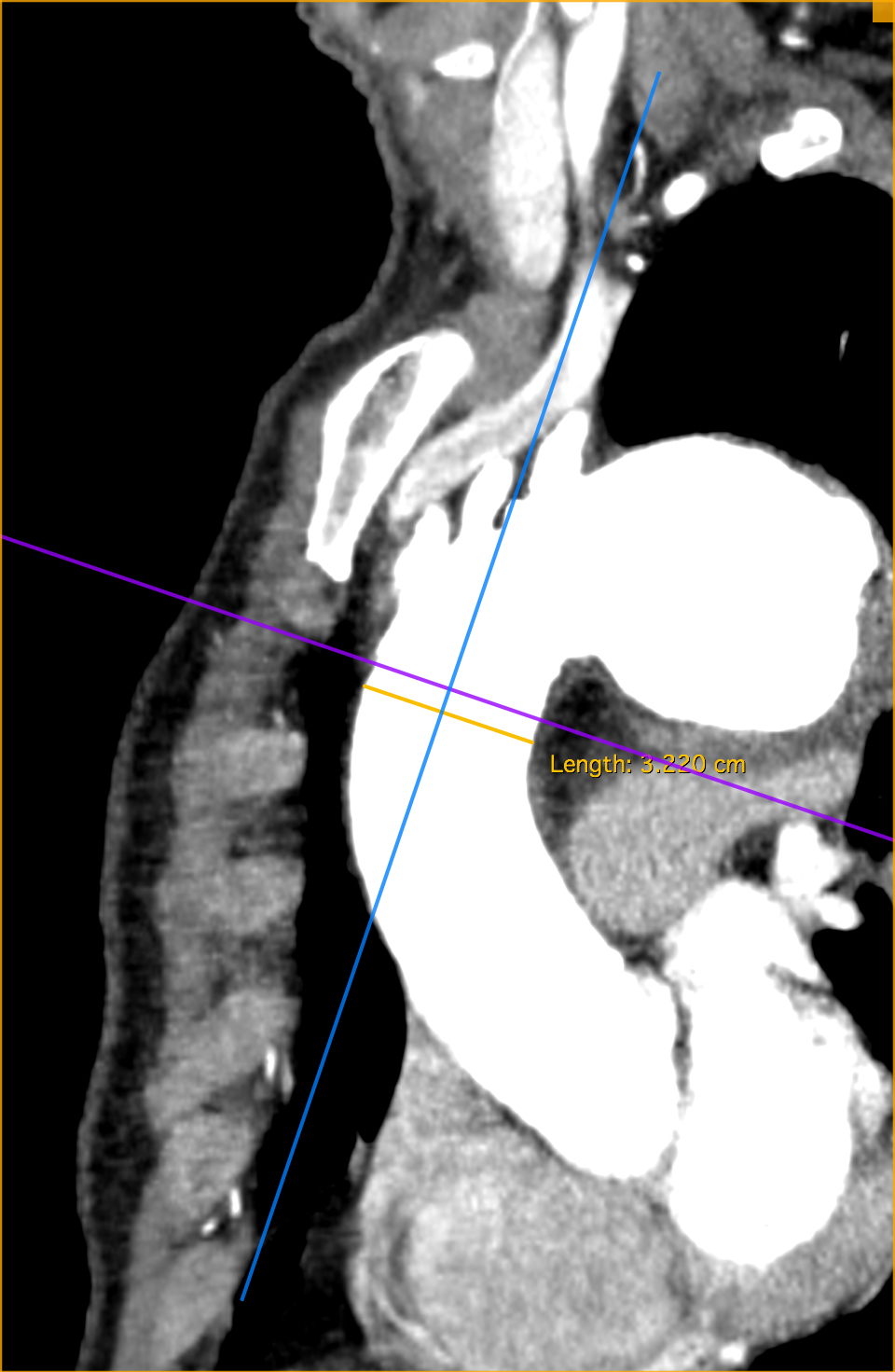
A man in his 60s, known for hypertension, COPD, andcoronary syndrome, seeks help due to chest pain. His blood pressure registers160/90, heart rate at 85. Imaging (CTA) highlights a concerning finding: anaortic arch aneurysm, extending into the left subclavian artery (LSA) with amaximum diameter of 6.8cm. The aneurysm exhibits a short proximal neck, withthe proximal landing zone measuring 3.2cm in diameter.

Relevant Test Results Prior to Catheterization
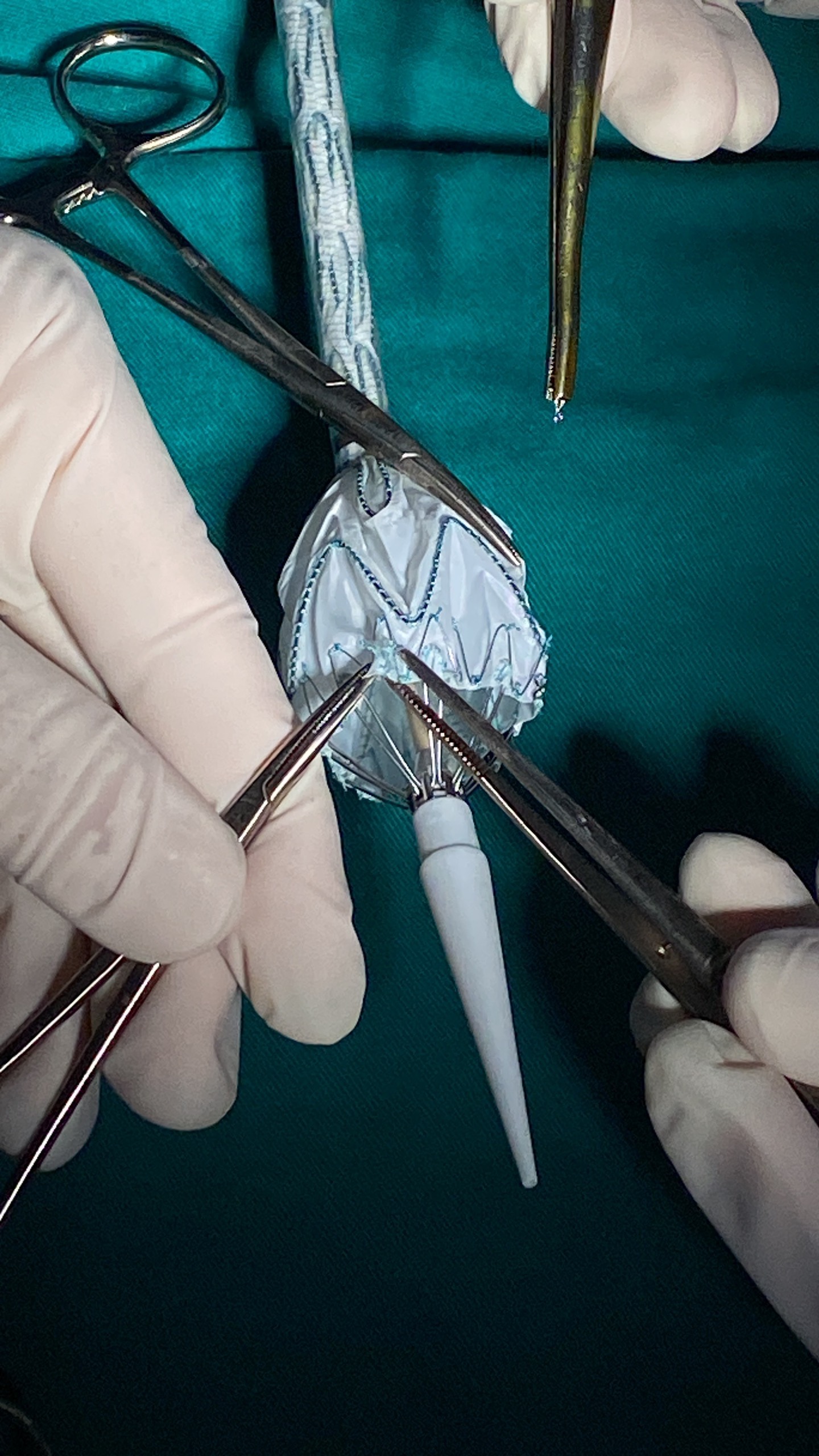
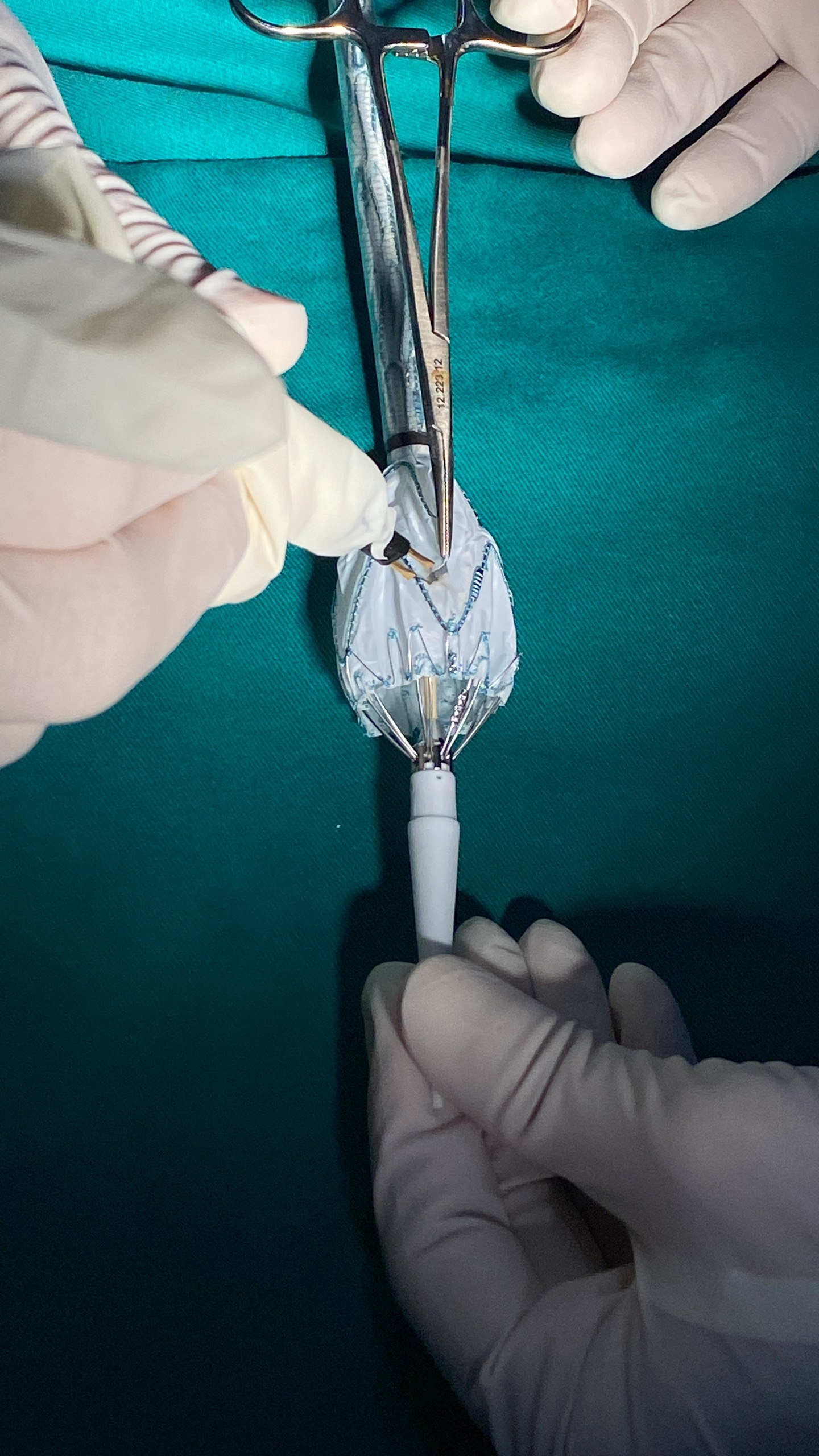
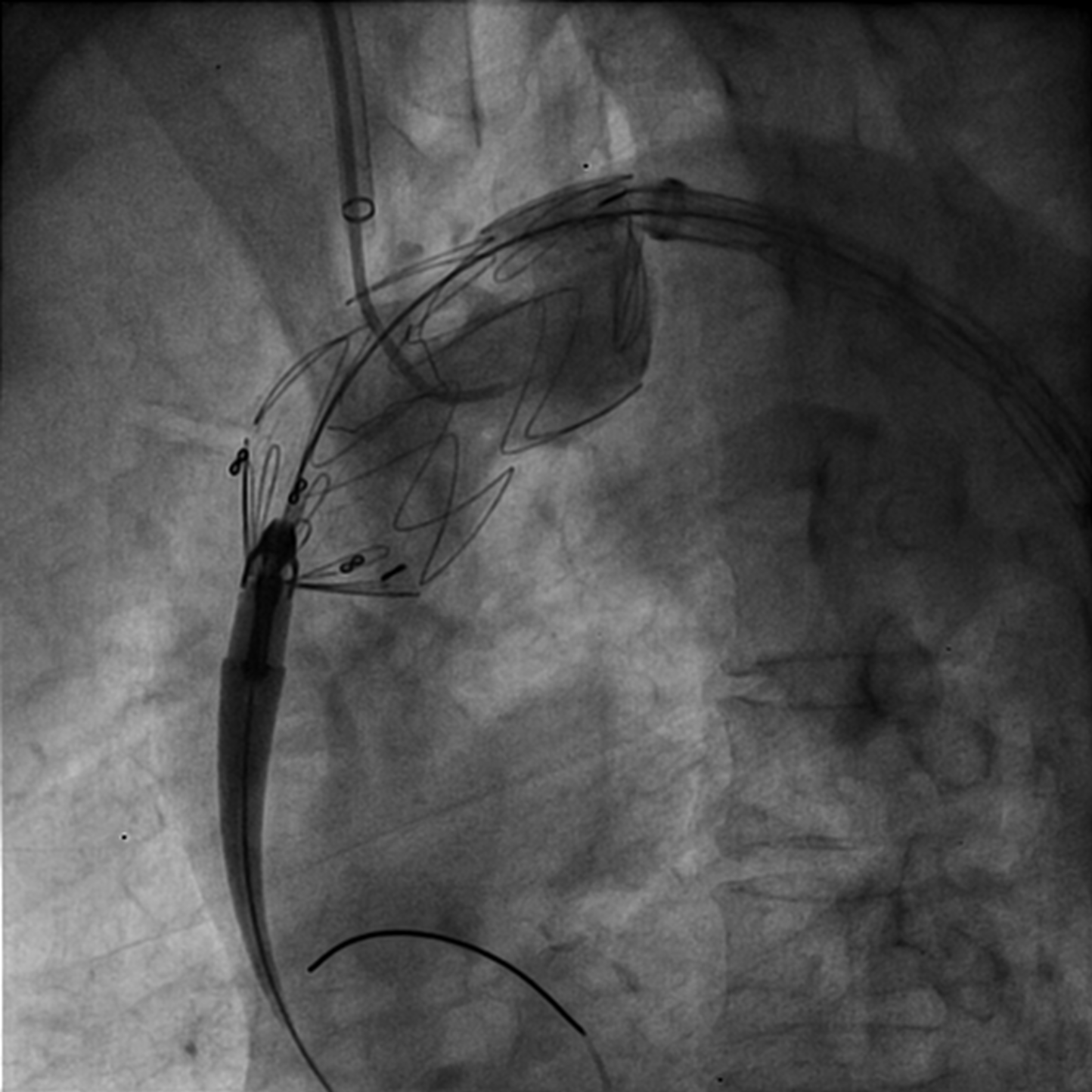
To create the fenestration for the innominate artery, aligning with the radiopaque figure-8 mid-body marker and figure-8 marker in the proximal edge stent graft. The distance between edge proximal Stent graft to fenestration is 20mm. At the proximal Valiant captiva Stent graft have 4 figure-8 marker, we cut 2 figure-8 marker at the both side of stent graft and sew figure-8 marker at the edge of fenestration (figure-8 marker at the edge proximal, 2 figure-8 marker at the edge of fenestration, figure-8 marker at the middle body stent graft in one line) (figure ) to facilitate relief where is fenestration

Relevant Catheterization Findings
Interventional Management
Procedural Step
In response to the urgent situation and considering the patient's comorbidities, we opted for a right-to-left carotid artery bypass followed by a single fenestration thoracic endovascular aortic repair (TEVAR).
Device preparation involved using a three-dimensional vascular imaging workstation (3mensio) for sizing and planning, deploying the stent graft partially to create a 12mm fenestration, aligning it precisely with the innominate artery orifice, using radiopaque figure-8 markers for guidance, and maintaining a 20mm distance between the proximal stent graft edge and the fenestration.
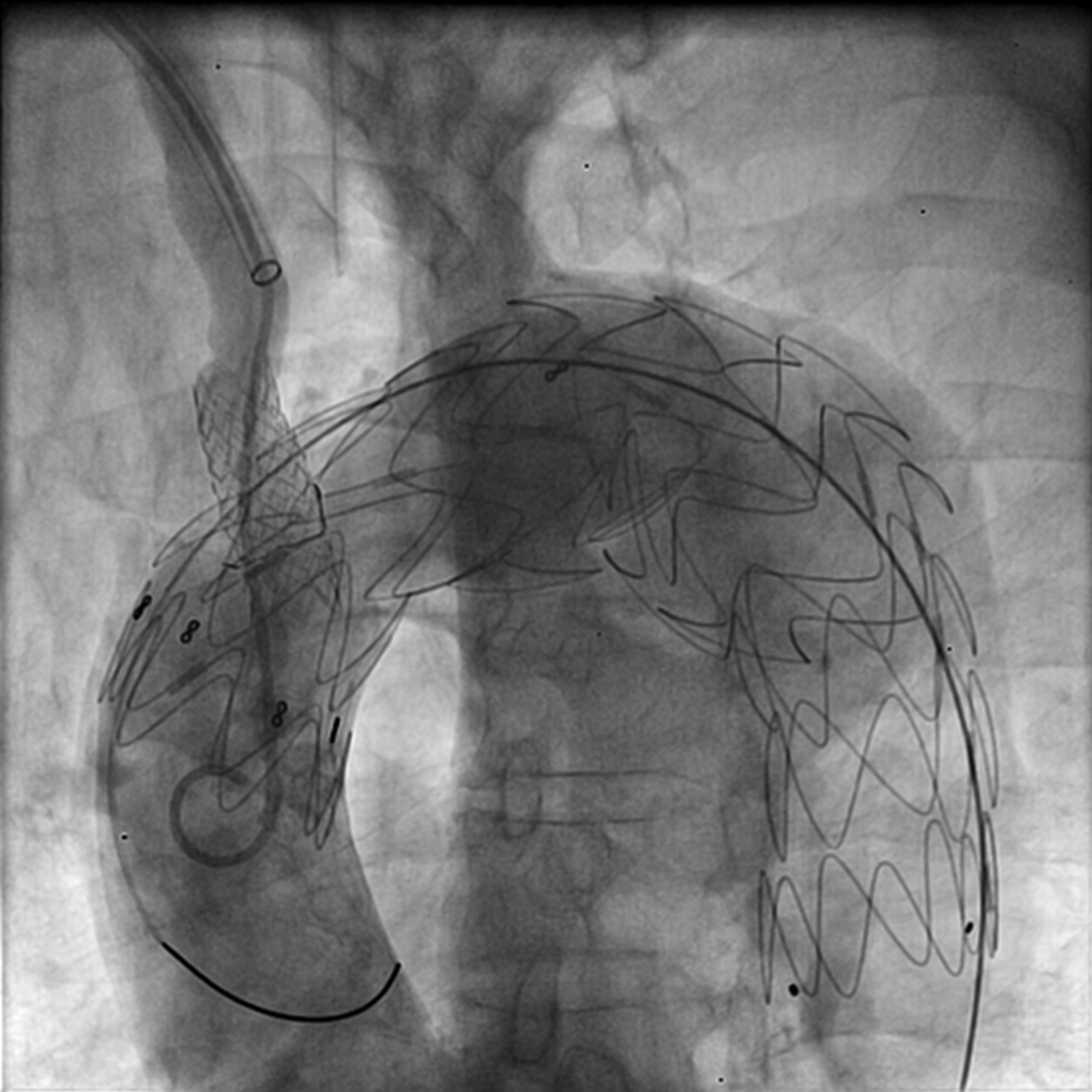
During the procedure, the image intensifier (LAO) was positioned to visualize the innominate artery origins optimally, showing its ostium arising from the greater curvature. The stent graft insertion, guided by a super-stiff wire, was rotated to ensure the fenestration's superior orientation upon entering the arch, aligning the figure-8 mid-body marker with the greater curvature. This positioning facilitated direct opposition of the innominate fenestration to its origin. Subsequently, catheter engagement from the innominate artery to the fenestration allowed for full stent graft deployment and cover stent inflation, ensuring protection of the innominate artery.
Postoperatively, the patient was discharged on day 10 without neurological deficits. A follow-up CTA six months later confirmed the patency of the endograft, carotid-carotid bypass, and innominate artery fenestration.

Device preparation involved using a three-dimensional vascular imaging workstation (3mensio) for sizing and planning, deploying the stent graft partially to create a 12mm fenestration, aligning it precisely with the innominate artery orifice, using radiopaque figure-8 markers for guidance, and maintaining a 20mm distance between the proximal stent graft edge and the fenestration.
During the procedure, the image intensifier (LAO) was positioned to visualize the innominate artery origins optimally, showing its ostium arising from the greater curvature. The stent graft insertion, guided by a super-stiff wire, was rotated to ensure the fenestration's superior orientation upon entering the arch, aligning the figure-8 mid-body marker with the greater curvature. This positioning facilitated direct opposition of the innominate fenestration to its origin. Subsequently, catheter engagement from the innominate artery to the fenestration allowed for full stent graft deployment and cover stent inflation, ensuring protection of the innominate artery.
Postoperatively, the patient was discharged on day 10 without neurological deficits. A follow-up CTA six months later confirmed the patency of the endograft, carotid-carotid bypass, and innominate artery fenestration.
Case Summary
The hybrid carotid-carotid bypass combined with on-table fenestrated innominate in zone 0 TEVAR for aortic arch aneurysm suits unfit patients avoiding open repair. The Vietnam National Heart Institute's method, using Self-Radiopaque Technique follow Aortic Curvature Guidance, streamlines the procedure. However, a broader case series and prolonged follow-up are crucial to confirm its safety and effectiveness.