
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-109
Decode and Deliver
By Kogulakrishnan Kaniappan, Azmee Mohd Ghazi
Presenter
Kogulakrishnan Kaniappan
Authors
Kogulakrishnan Kaniappan1, Azmee Mohd Ghazi1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-109
Coronary - Complication Management
Decode and Deliver
Kogulakrishnan Kaniappan1, Azmee Mohd Ghazi1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
56 yearsold Male
On examination, Well, not tachypnoeicBP : 130 /80 mm HgHR : 100 bpmSpo2 : 98% on room airLungs : ClearCVS : DRNMNo pedal edema
- IHD – PCI to LAD 2015
- HPT
- DM
- Dyslipidemia
On examination, Well, not tachypnoeicBP : 130 /80 mm HgHR : 100 bpmSpo2 : 98% on room airLungs : ClearCVS : DRNMNo pedal edema
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
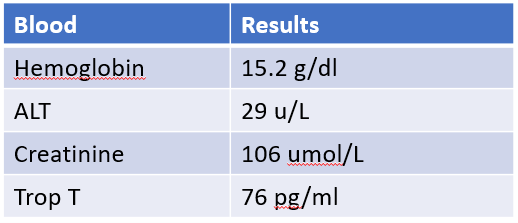
Coronary angiogram :
Left Main Stem : normalLAD : Patent stent , mild diseaseLCX : mild diseaseRCA : Anomalous origin, tight stenosis at mid segment

Left Main Stem : normalLAD : Patent stent , mild diseaseLCX : mild diseaseRCA : Anomalous origin, tight stenosis at mid segment
Interventional Management
Procedural Step
QFR RCA was 0.76 ( Significant lesion )

Case Summary
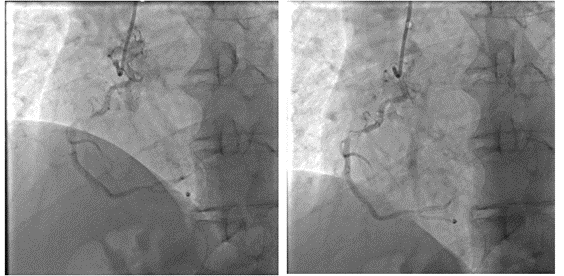
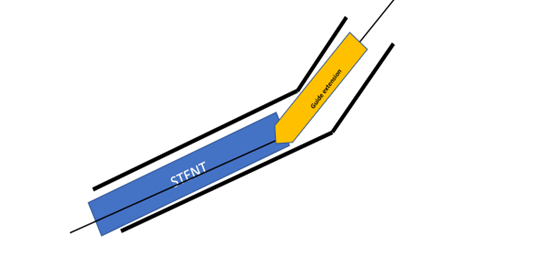
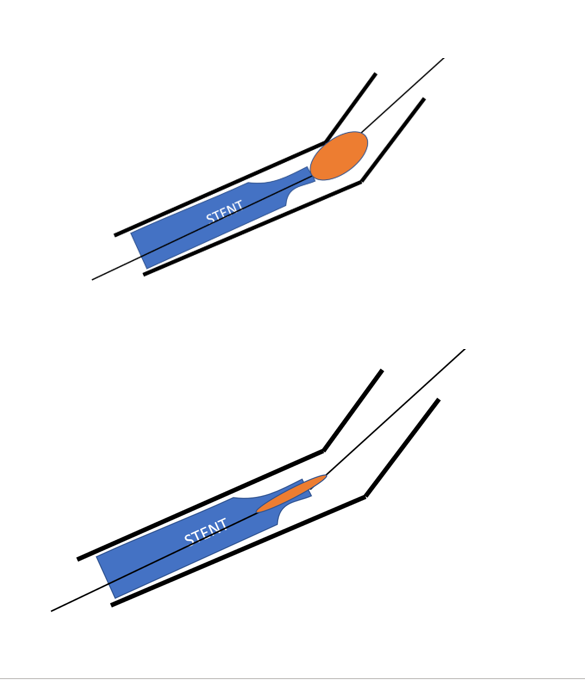
1. Anomalous RCA angioplastyrequires good guide support for co-axial engagement and to advance devices