
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-087
LM Bifurcation With Rotatrypsy in 75 Yr Old Man With CKD
By Sumanta Shekhar Padhi
Presenter
Sumanta Shekhar Padhi
Authors
Sumanta Shekhar Padhi1
Affiliation
Raipur- MMI Narayana Superspeciality Hospital, India1,
View Study Report
TCTAP C-087
Coronary - Complex PCI - Left main
LM Bifurcation With Rotatrypsy in 75 Yr Old Man With CKD
Sumanta Shekhar Padhi1
Raipur- MMI Narayana Superspeciality Hospital, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
75yr /M/Long standingDM and HTN, presented with NSTEMI, Moderate LV dysfunction- EF- 35-40% & LVFHe is known case of CKD with Cr of ~2.6.
Relevant Test Results Prior to Catheterization
On evaluation had moderate LV dysfunction. TheLAD territory hypokinetic. EF 35-40%.. Creatinine afterstabilization- 2.6mg/dl. B/L shrunken kidneys by USG
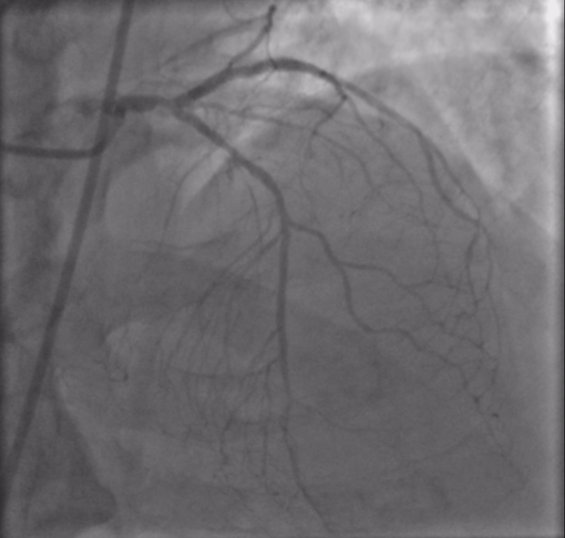
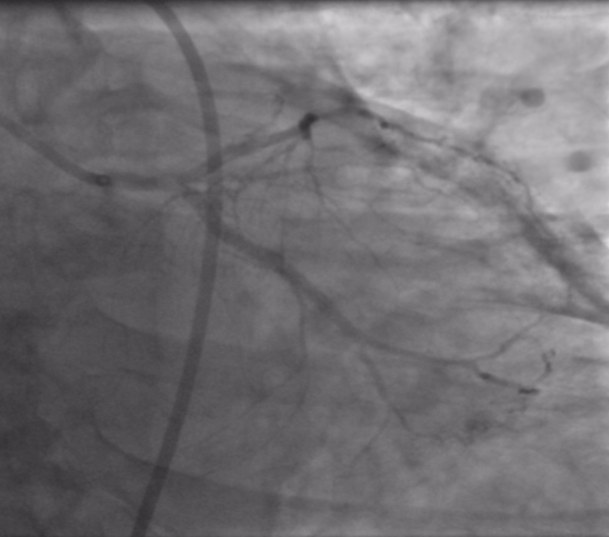
Relevant Catheterization Findings
CAG done after stabilization showed: LMCA bifurcation disease: Medina 1,0,1.Large chunk of calcium just at bifurcation. Distal LAD- diffusely disease. Proximal edge of LCX stent and ostium of LCX significantly diseased. RCA – proximal CTO. Plan of treatment :CABG( MICS)- LIMA to LAD and graft to OM. However, relatives refused in v/o age


Interventional Management
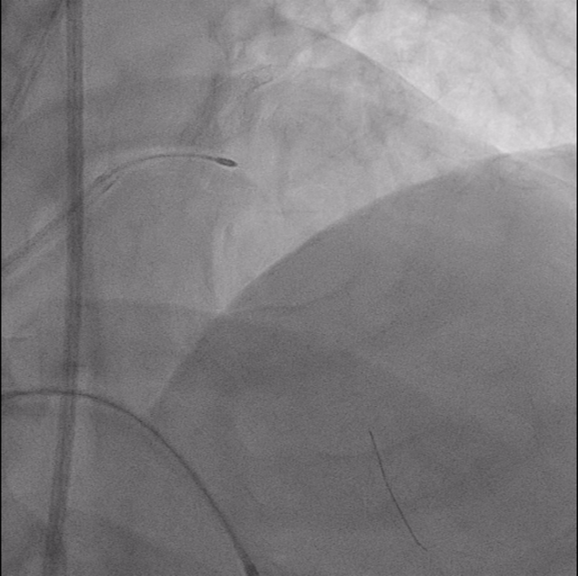
Procedural Step
PCI was planned: LMCA bifurcation, Two stent strategy-TAP, Calciumreduction technique (IVL and ROTA),IVUS and TPI. IABP- standby. Accesses- RFA-7F,RVF-7F-for TPI ,6F LFA-6F for IABP ( stand by)


Case Summary
Post procedure pt’s course was complicated by hematoma in Rtgroin requiring 1 unit of BT. He also had LVF and hypotension. It was managedconservatively, But pt’s hospital stay was prolonged and could be discharged 2 week after the procedure.