
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-059
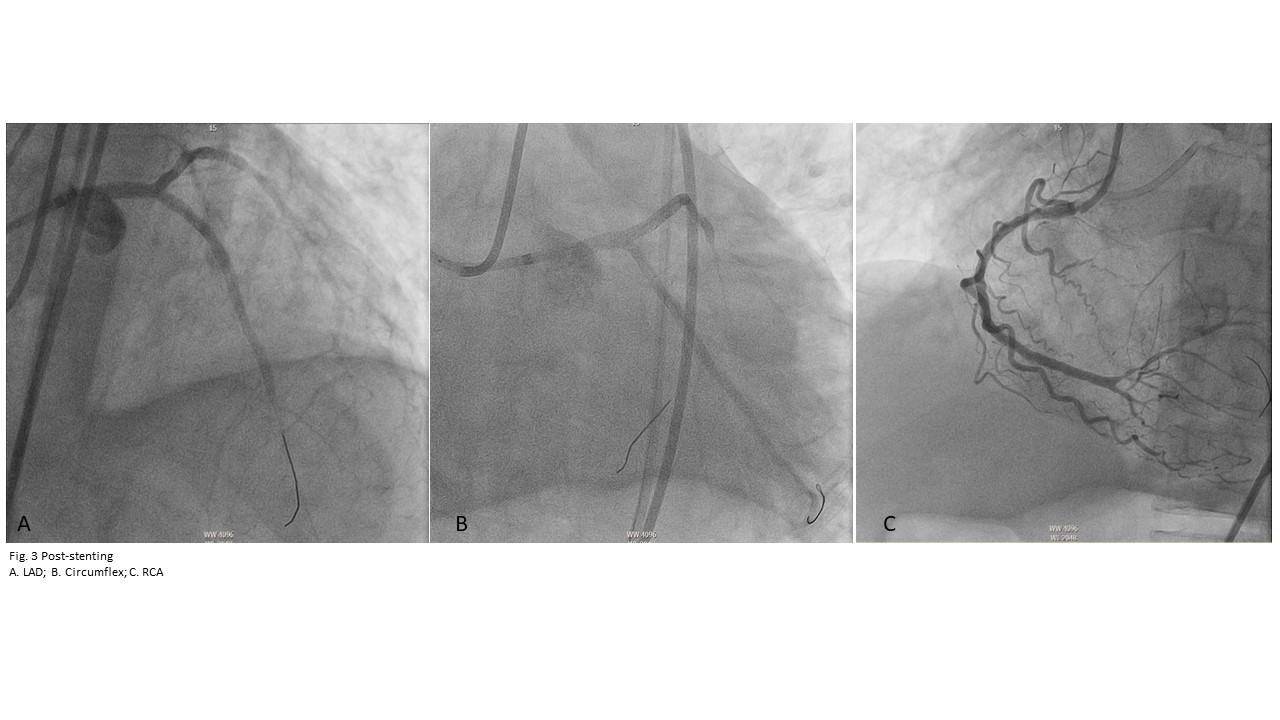
"Double Trouble": Antegrade and Retrograde Approach in Chronic Total Occlusion of the Right Coronary Artery and Left Anterior Descending Artery
By Ronaldo Estacio, Jemilyn Valenzuela Bandillo
Presenter
Jemilyn Valenzuela Bandillo
Authors
Ronaldo Estacio1, Jemilyn Valenzuela Bandillo1
Affiliation
Philippine Heart Center, Philippines1,
View Study Report
TCTAP C-059
Coronary - Complex PCI - CTO
"Double Trouble": Antegrade and Retrograde Approach in Chronic Total Occlusion of the Right Coronary Artery and Left Anterior Descending Artery
Ronaldo Estacio1, Jemilyn Valenzuela Bandillo1
Philippine Heart Center, Philippines1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
ML, a 67 year old Filipino, male a known case of 3 vessel coronary artery disease with totally occluded LAD, RCA and a known CKD on hemodialysis. Few hours prior to admission patient had chest pain with hypotension and was managed as case of NSTE-ACS. He underwent coronary angiogram which showed the same lesion . He was advised CABG but due to high surgical risk and patient’s consent, he underwent percutaneous coronary intervention.
Relevant Test Results Prior to Catheterization
Transthoracic echocardiogram showed low ejection fraction with segmentalwall motion abnormality. EURO score is 5.92. Creatinine is 3.28 mg/dl
Relevant Catheterization Findings
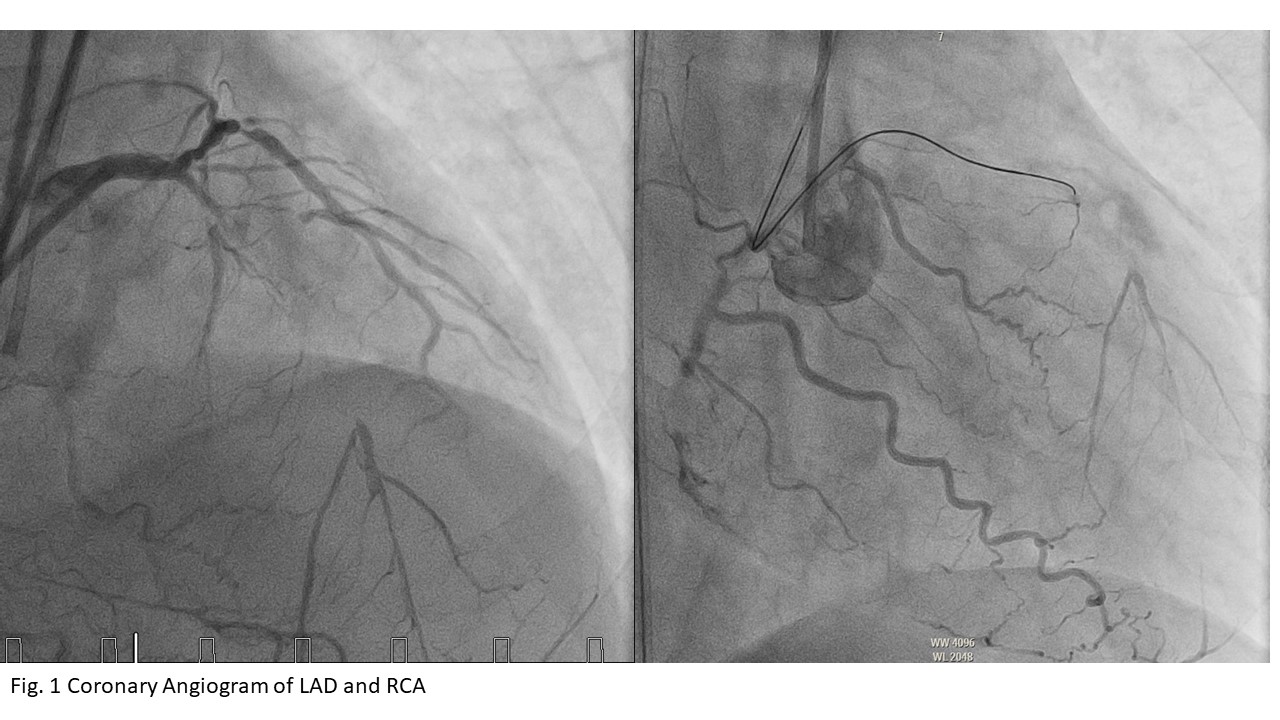
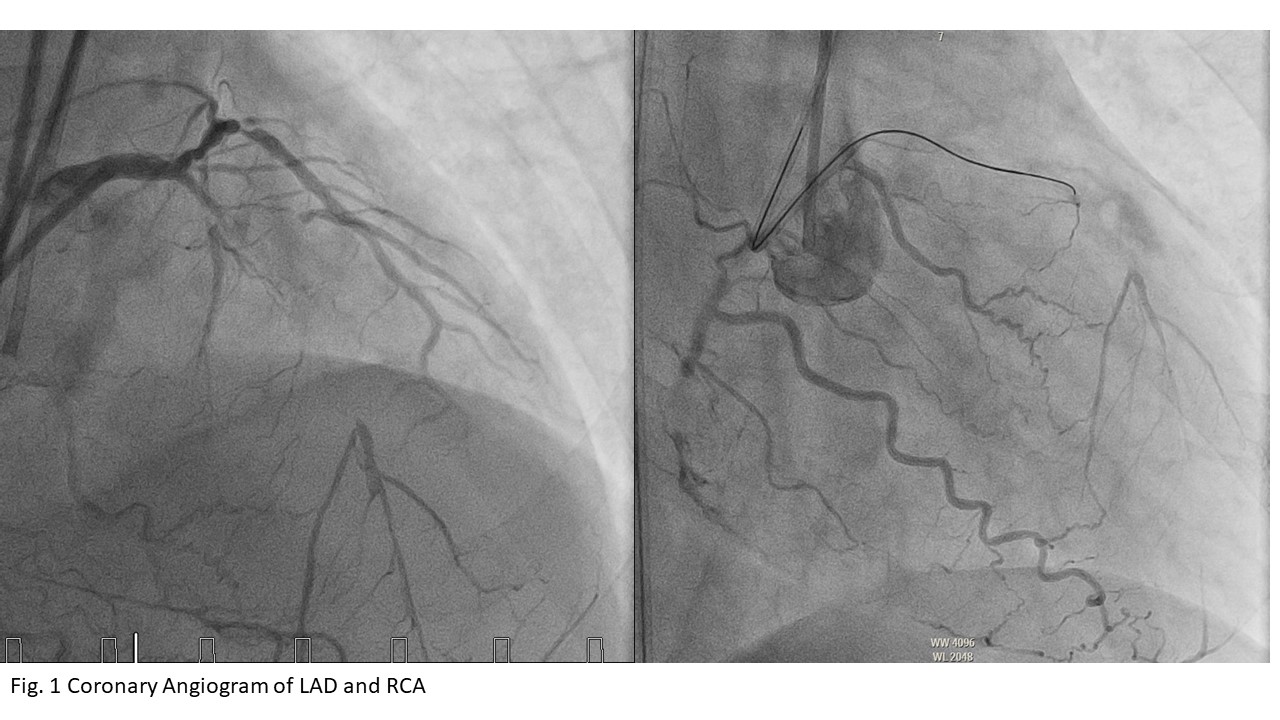
The coronary angiogram showed the a totally occluded left anterior descending artery at the proximal segment, the more distal segment is visualized via right to left collaterals. The circumflex is non-dominant with 70% stenosis. The RCA is totally occluded at the mid segment and the distal vessel is visualized via right to right collaterals.

Interventional Management
Procedural Step
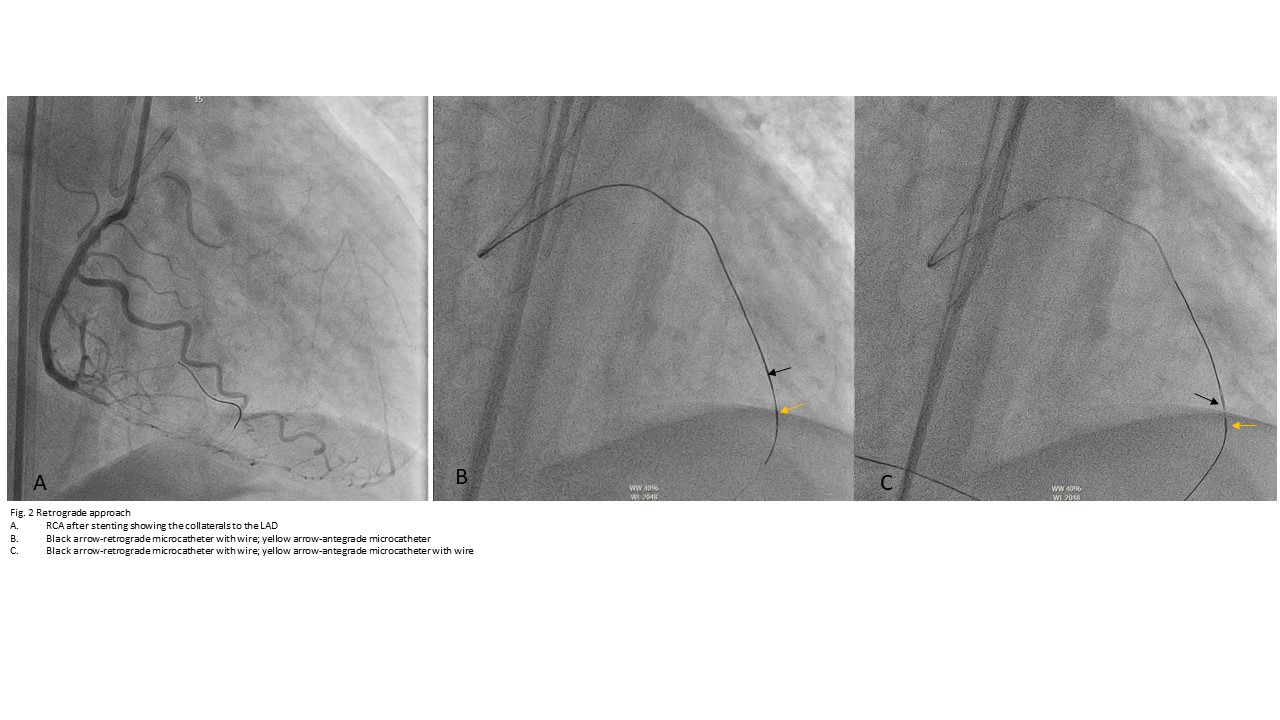
Dual injection in the left and right coronary artery systems was used to visualized antegrade and retrograde flow to LAD. Initially, antegrade approach was done but failed to cross the CTO of the LAD after multiple attempts. We then proceeded with crossing the CTO of the RCA using a Caravel Microcatheter with Asahi Blue exchanged with Conquest Pro 12 which crossed lesion. After crossing and stenting the CTO of the RCA, the RPDA to the septal perforator was used in the retrograde technique. Initially, Asahi Sion with Caravel Asahi microcatheter was used and was exchanged with Asahi Suoh 3 then Asahi Sion Black up to the distal LAD and was exchanged with Asahi Ultimatebros 3, Asahi Gladius EX14 and finally Asahi Conquest Pro 12 was able to puncture the proximal cap of the CTO retrogradely. The retrograde Caravel was unable to advance more proximally into the LAD, hence, Conquest Pro 12 was advanced in the antegrade Asahi Corsair Pro XS thru the left guide catheter. The Corsair XS Pro was advanced to the distal LAD to meet tip to tip with Asahi Caravel up to the distal LAD. The Conquest Pro 12 was withdrawn slowly while advancing the Runthrough Hypercoat Terumo thru the antegrade microcatheter to the distal LAD. The retrograde wire and microcather was removed then proceeded with successful stenting of the LAD. The circumflex artery was stented prior to stenting the Left main to proximal LAD.
Case Summary
Coronary artery bypass graft is still the recommended procedure for 3 vessel coronary artery disease with left main involvement. However, we have to assess individual risks and how complicated the procedure will be. If complex percutaneous coronary intervention will be the choice, patient should understand the risks as well as the chance of failure and success especially in very difficult cases.