
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-187
Anomalous Coronary Artery Origin Presenting Clinically as a Chronic Coronary Syndrome: A Case Report
By Kevin Francio, Putu Dwipa Krisna Devi, Rosi Amrilla Fagi, Budi PIkir
Presenter
Kevin Francio
Authors
Kevin Francio1, Putu Dwipa Krisna Devi2, Rosi Amrilla Fagi1, Budi PIkir3
Affiliation
Universitas Airlangga, Dr Soetomo General Hospital, Indonesia1, Universitas Airlangga, Indonesia2, Universitas Airlangga, Dr Soetomo General Hospital, Indonesia, Indonesia3,
View Study Report
TCTAP C-187
Coronary - Imaging & Physiology - Non-Invasive Imaging (CTA, MRI, Echo, etc)
Anomalous Coronary Artery Origin Presenting Clinically as a Chronic Coronary Syndrome: A Case Report
Kevin Francio1, Putu Dwipa Krisna Devi2, Rosi Amrilla Fagi1, Budi PIkir3
Universitas Airlangga, Dr Soetomo General Hospital, Indonesia1, Universitas Airlangga, Indonesia2, Universitas Airlangga, Dr Soetomo General Hospital, Indonesia, Indonesia3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
60 years old woman was referred to cardiology outpatient clinic because of frequent chest pain since 8 years ago. The chest pain classified using Canadian Cardiovascular Society (CCS) anginal class as class II and was relieved by resting or taking nitrates. Patient's risk factor was hypertension and dyslipidemia, with no history of acute coronary syndrome episodes.
Patient's daily blood pressure was around 130-140/70-90 mmHg, with resting heart rate at around 60 beats per minute
Patient's daily blood pressure was around 130-140/70-90 mmHg, with resting heart rate at around 60 beats per minute
Relevant Test Results Prior to Catheterization
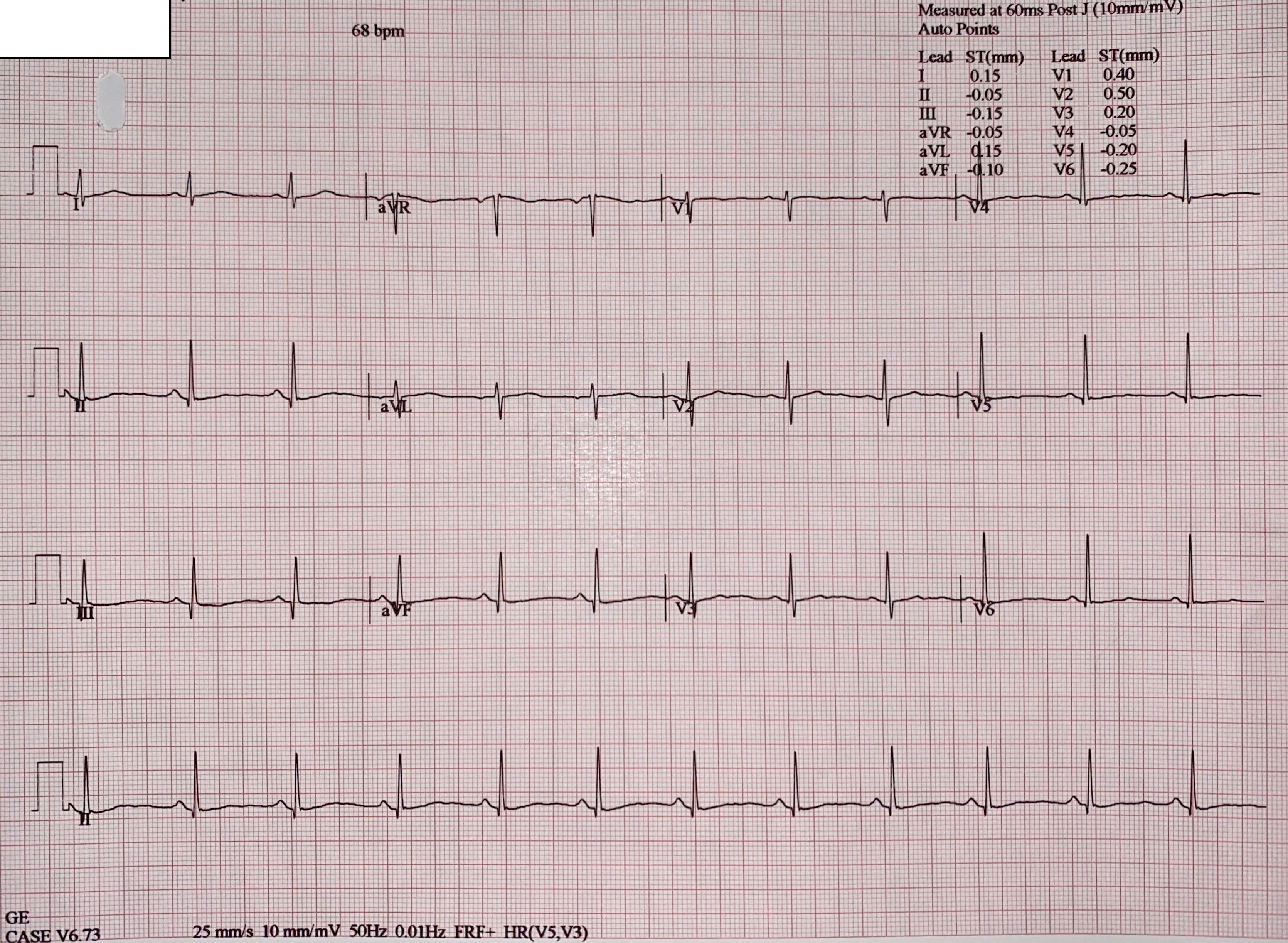
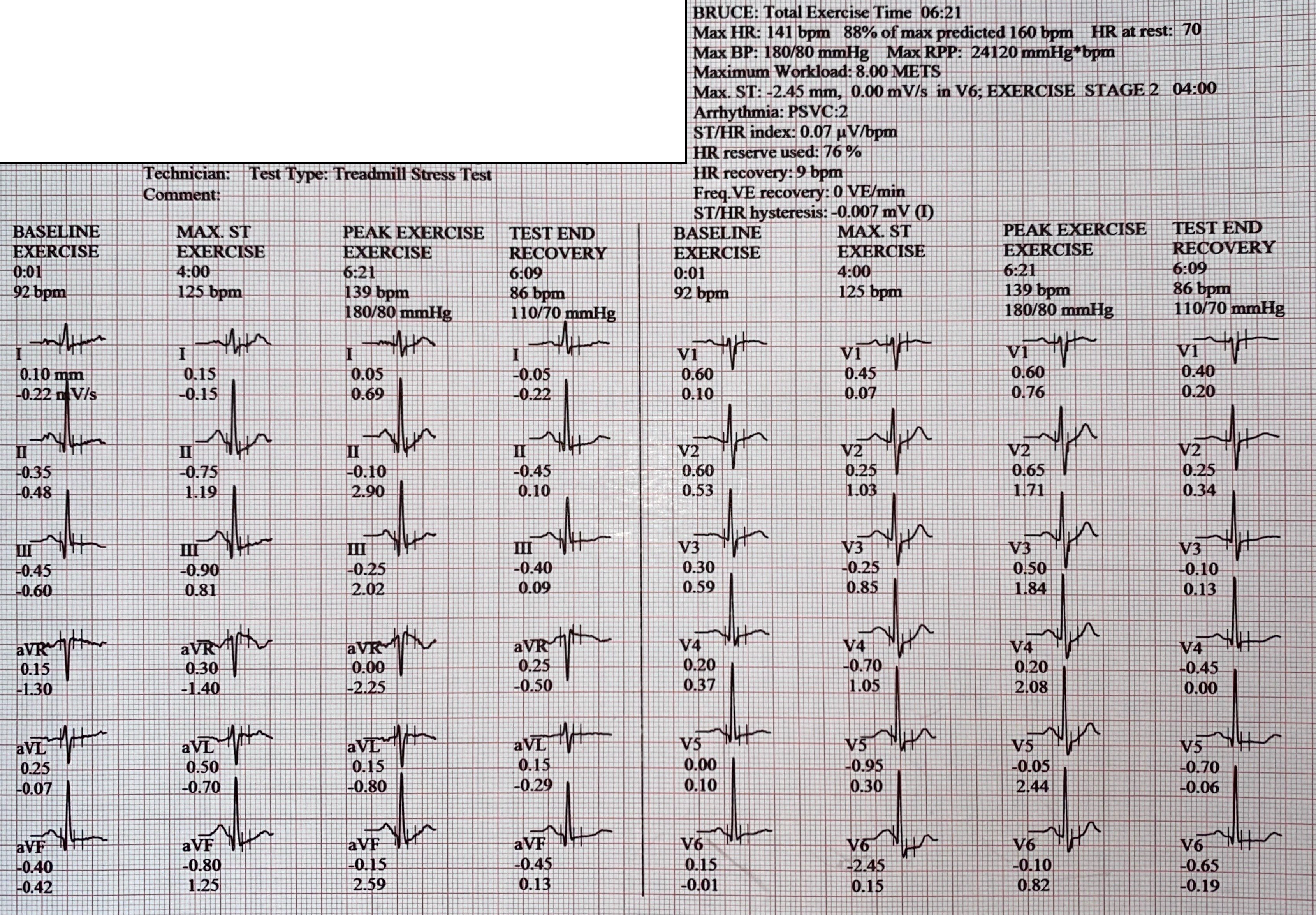
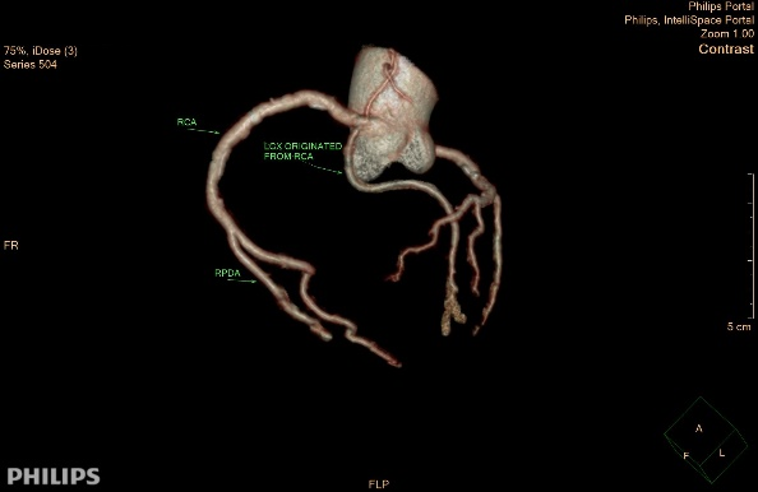
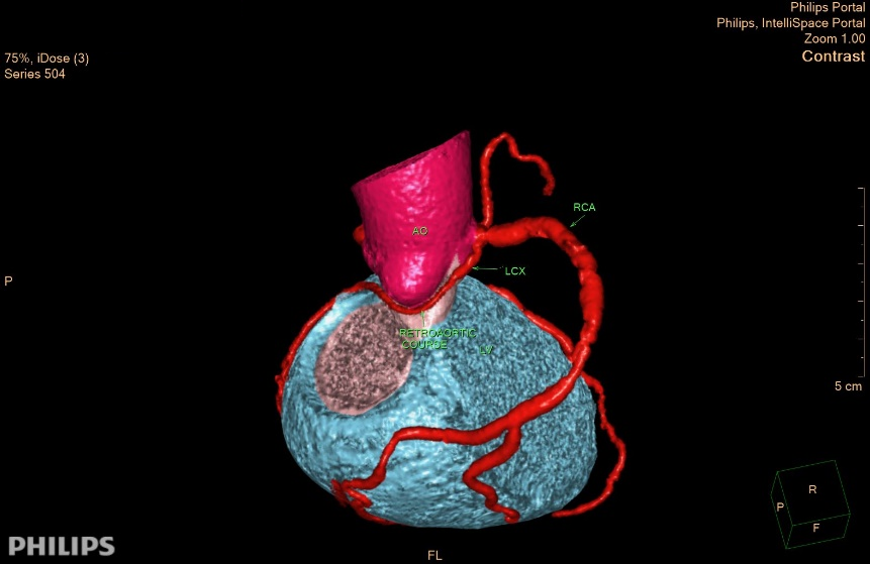
Baseline ECG was normal. Echocardiography showed preserved LV ejection fraction without any regional wall motion abnormalityTreadmill Exercise Stress Test were suggestive of ischemia with upsloping ST segment depression at inferior and anterolateral leadsCT Coronary Angiography showed coronary artery anomalous origin, LCx was from proximal part of RCA with retro-aortic course with. Agatston score of 489 with mild stenosis at LAD, LCx, and RCA
Relevant Catheterization Findings
Cannulation to Left Main Coronary Artery showed no Left Circumflex Artery was found. There was non significant stenosis at proximal part of Left Anterior Descending Artery.
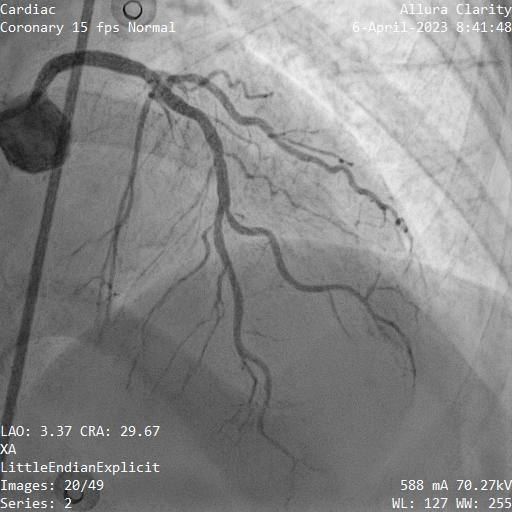
Cannulation to Right Coronary Artery showed a vessel with ostium with acute take-off angle at the proximal part of RCA, coursing through the course of an Left Circumflex Artery with small diameter. The RCA had non significant stenosis at mid to distal part


Interventional Management
Procedural Step
CT Coronary Angiography was done using a MSCT 128 slices performed with retrospective ECG gating. Contrast used was Xolmetras 75 cc given at 5.0 cc/second followed by saline. Image quality was good, with patient heart rate was 60 beats per minutes
Diagnostic invasive coronary angiography was done by femoral access, using JL 4.0 6F Catheter for LMCA cannulation and JR 4.0 6F Catheter for RCA cannulation. During RCA cannulation, the tip of catheter needs to be placed at the very ostium of RCA to be able to visualize the LCx due to its acute take-off angle. At the first angioraphy, the JR catheter was inserted too much into RCA and the anomalous LCx cannot be viewed clearly. JR Catheter was then pulled to near of ostium so the LCx can be visualized clearly. Contrast used was Ultravist
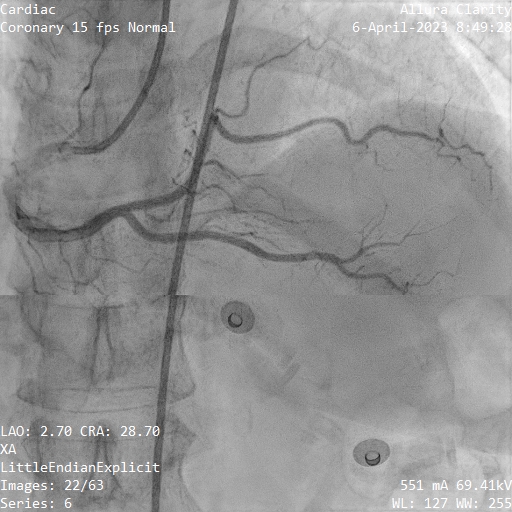


Diagnostic invasive coronary angiography was done by femoral access, using JL 4.0 6F Catheter for LMCA cannulation and JR 4.0 6F Catheter for RCA cannulation. During RCA cannulation, the tip of catheter needs to be placed at the very ostium of RCA to be able to visualize the LCx due to its acute take-off angle. At the first angioraphy, the JR catheter was inserted too much into RCA and the anomalous LCx cannot be viewed clearly. JR Catheter was then pulled to near of ostium so the LCx can be visualized clearly. Contrast used was Ultravist
Case Summary
This patient had anomalous origin from opposite sinus (ACAOS). Left Circumflex Coronary Artery was found arising from the proximal part of Right Coronary Artery with retro-aortic course, anatomically categorized as benign and low riskDespite being benign and low risk ACAOS without any significant stenosis found, patient still complained angina on effort with functional testing using exercise stress testing showed suggestive result of ischemiaWe suspected the acute take-off angle of the LCx from RCA, causing kinking of the proximal part of LCx as the possible culprit mechanism inducing ischemia.