
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-030
IVUS Guided Non Left Main DK-Crush Stenting (LAD/D1) Bifurcation
By Kala Jeethender Kumar
Presenter
Kala Jeethender Kumar
Authors
Kala Jeethender Kumar1
Affiliation
Yashoda Hospitals Hi-Tech City, India1,
View Study Report
TCTAP C-030
Coronary - Complex PCI - Bifurcation
IVUS Guided Non Left Main DK-Crush Stenting (LAD/D1) Bifurcation
Kala Jeethender Kumar1
Yashoda Hospitals Hi-Tech City, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
45 years old male known hypertensive presented with chest pain associated with exertional shortness of breath on and off since 1week. CAD-Un stable angina. On Examination-PR-78/min, BP-110/70mmHg, RR-20/min, SPO2-96%, CVS-S1+, S2+, P/A-Soft BS+, RS-Bilateral air entry adequate, CNS-No focal neurological deficit. Investigations-Hb-14.4g/dl, Serum creatinine-0.76mg/dl, RBS-135mg/dl.

Relevant Test Results Prior to Catheterization
ECG showed NSR, 2D Echo revealed RWMA+ in LAD territory, hypokinetic, good LV function, EF-60%.
Relevant Catheterization Findings
Coronary angiogram revealed Single vessel disease, LMCA-Normal, LAD-proximal 50-60% lesion, mid LAD 90% lesion at diagonal, LCX-Normal, RCA-Normal.

Interventional Management
Procedural Step
Procedure performed through right radial artery LMCA engaged with 7Fr EBU 3.5 Guiding catheter which showed LAD-proximal 50-60% lesion, mid LAD 90% lesion at diagonal. 0.014x180cm Run through wire placed in LAD, another wire placed in D1. LAD predilatation done with 2.0x12mm Balloon. Pre procedure IVUS study showed mid LAD 2.72sqmm with fibrous fatty plaque with 600 calcium, proximal LAD 2.81sqmm with fibrous fatty plaque and D1 1.64sqmm with fibrous fatty plaque. D1 stenting done with 2.5x15mm DES. LAD predilatation done with 3.5x12mm Balloon. D1 postdilatation done with 1.25x10mm, 2.0x8mm 2.5x12mm Balloons. First KBT done with 2.5x12mm balloon in D1, 3.5x12mm balloon in LAD. LAD stenting done with 3.0x48mm DES. LAD post dilatation done with 3.5x12mm balloon. Diagonal stent crushed. Proximal LAD post dilatation done with 4.0x12mm balloons. LAD post dilatation done with 1.25x8mm, 2.0x8mm, 2.5x12mm balloons. Final kissing balloon dilatation done with 2.5x12mm balloon in D1, 4.0x12mm balloon in LAD. POT of LAD done with 4.0x12mm balloon. Post procedure IVUS showed distal segment 5.93sqmm, mid segment 12.05sqmm, proximal segment 11.8sqmm and well apposed stent struts and no residual stenosis. The final result was good with TIMI III Flow without any Complications. Patient was discharged in a stable status on 3rd post procedure day without any CV Symptoms.

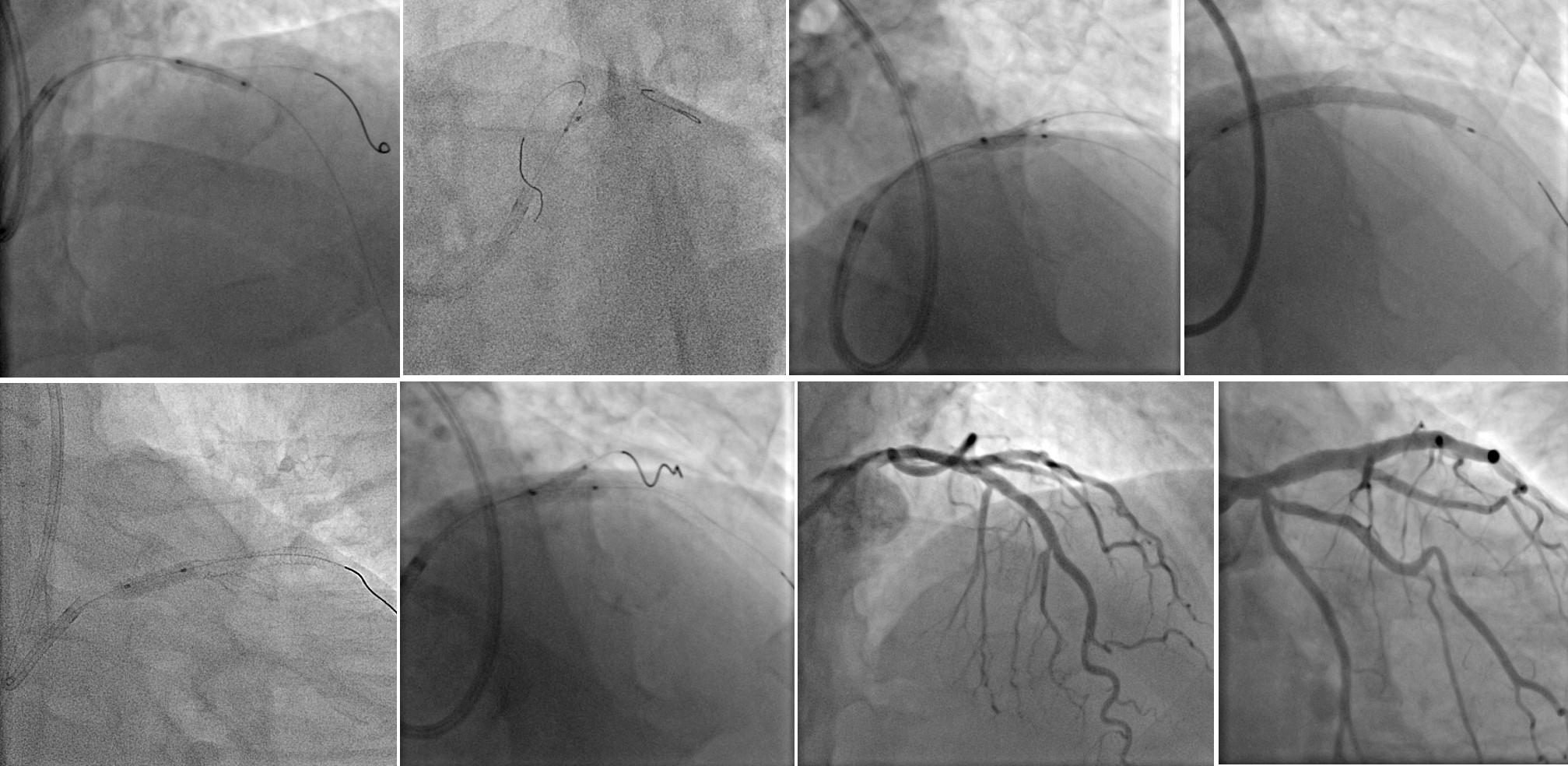
Case Summary
DK crush appears to be the ‘real deal’ with the best clinical outcomes in true complex bifurcation disease requiring an up-front 2-stent strategy. the DK crush technique is superior to the PS technique for complex bifurcation lesions, with a significant reduction in MACE, TVMI, and rates of revascularization. The DK crush stenting provides the best evidence-based approach to complex bifurcation lesions especially LM and LAD/D1 bifurcation lesions. Pre and Post PCI IVUS was used for optimization of PCI.